Gaurav Pandey, Salman Pervaiz Butt, Arshad Ghori, Naveen G Singh
{"title":"经皮无创血气分析监测小儿心脏手术患者拔管后气体交换的评价。","authors":"Gaurav Pandey, Salman Pervaiz Butt, Arshad Ghori, Naveen G Singh","doi":"10.21470/1678-9741-2024-0010","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Pediatric cardiac surgery patients need close post-extubation monitoring for ventilation. Non-invasive transcutaneous partial pressure of oxygen (TcPO2) and transcutaneous partial pressure of carbon dioxide (TcPCO2) offer continuous insights and in improving care.</p><p><strong>Objective: </strong>To investigate the correlation of transcutaneous blood gases (TcPO2, TcPCO2) with arterial blood gases i.e. arterial partial pressure of oxygen (PaO2) and arterial partial pressure of carbon dioxide (PaCO2).</p><p><strong>Methods: </strong>We conducted a study on 30 pediatric post-cardiac surgery patients (four months to three years old) who were extubated and exhibited stable hemodynamics (inotropic score ≤ 5), normal sinus rhythm, and no respiratory or heart failure signs. Continuous transcutaneous and intermittent arterial blood gas monitoring started one hour after extubation, with recordings every 30 minutes for four hours. A single observer conducted probe calibration and data recording to minimize variability, while analysis of 240 paired samples included correlation coefficient, linear regression, Bland-Altman analysis, and Mountain plot.</p><p><strong>Results: </strong>The r-value between PaCO2 and TcPCO2 was 0.95, r2-value of 0.9060 (P<0.001). Bland-Altman showed a bias of 2.579, and 95% limits of agreement were -6.4 to 1.3. The r-value between PaO2 and TcPO2 was 0.8942, r2-value of 0.7996 (P<0.001); bias of 20.171 and 95% limit of agreement of -0.5 to 40.9. The Mountain plot revealed a median of 2.57 for PaCO2 vs. TcPCO2 and 20.17 for PaO2 vs. TcPO2.</p><p><strong>Conclusion: </strong>Transcutaneous carbon dioxide values are interchangeable with arterial PaCO2 in our population study, acting as a surrogate in postoperative pediatric cardiac surgery. Confirmation with arterial blood gases is needed if discrepancies occur.</p>","PeriodicalId":72457,"journal":{"name":"Brazilian journal of cardiovascular surgery","volume":"40 3","pages":"e20240010"},"PeriodicalIF":1.2000,"publicationDate":"2025-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11952150/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of Transcutaneous Non-Invasive Blood Gas Analysis for Monitoring Gas Exchange in Pediatric Cardiac Surgical Patients Post Extubation.\",\"authors\":\"Gaurav Pandey, Salman Pervaiz Butt, Arshad Ghori, Naveen G Singh\",\"doi\":\"10.21470/1678-9741-2024-0010\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Pediatric cardiac surgery patients need close post-extubation monitoring for ventilation. Non-invasive transcutaneous partial pressure of oxygen (TcPO2) and transcutaneous partial pressure of carbon dioxide (TcPCO2) offer continuous insights and in improving care.</p><p><strong>Objective: </strong>To investigate the correlation of transcutaneous blood gases (TcPO2, TcPCO2) with arterial blood gases i.e. arterial partial pressure of oxygen (PaO2) and arterial partial pressure of carbon dioxide (PaCO2).</p><p><strong>Methods: </strong>We conducted a study on 30 pediatric post-cardiac surgery patients (four months to three years old) who were extubated and exhibited stable hemodynamics (inotropic score ≤ 5), normal sinus rhythm, and no respiratory or heart failure signs. Continuous transcutaneous and intermittent arterial blood gas monitoring started one hour after extubation, with recordings every 30 minutes for four hours. A single observer conducted probe calibration and data recording to minimize variability, while analysis of 240 paired samples included correlation coefficient, linear regression, Bland-Altman analysis, and Mountain plot.</p><p><strong>Results: </strong>The r-value between PaCO2 and TcPCO2 was 0.95, r2-value of 0.9060 (P<0.001). Bland-Altman showed a bias of 2.579, and 95% limits of agreement were -6.4 to 1.3. The r-value between PaO2 and TcPO2 was 0.8942, r2-value of 0.7996 (P<0.001); bias of 20.171 and 95% limit of agreement of -0.5 to 40.9. The Mountain plot revealed a median of 2.57 for PaCO2 vs. TcPCO2 and 20.17 for PaO2 vs. TcPO2.</p><p><strong>Conclusion: </strong>Transcutaneous carbon dioxide values are interchangeable with arterial PaCO2 in our population study, acting as a surrogate in postoperative pediatric cardiac surgery. Confirmation with arterial blood gases is needed if discrepancies occur.</p>\",\"PeriodicalId\":72457,\"journal\":{\"name\":\"Brazilian journal of cardiovascular surgery\",\"volume\":\"40 3\",\"pages\":\"e20240010\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11952150/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Brazilian journal of cardiovascular surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21470/1678-9741-2024-0010\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brazilian journal of cardiovascular surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21470/1678-9741-2024-0010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Evaluation of Transcutaneous Non-Invasive Blood Gas Analysis for Monitoring Gas Exchange in Pediatric Cardiac Surgical Patients Post Extubation.
Introduction: Pediatric cardiac surgery patients need close post-extubation monitoring for ventilation. Non-invasive transcutaneous partial pressure of oxygen (TcPO2) and transcutaneous partial pressure of carbon dioxide (TcPCO2) offer continuous insights and in improving care.
Objective: To investigate the correlation of transcutaneous blood gases (TcPO2, TcPCO2) with arterial blood gases i.e. arterial partial pressure of oxygen (PaO2) and arterial partial pressure of carbon dioxide (PaCO2).
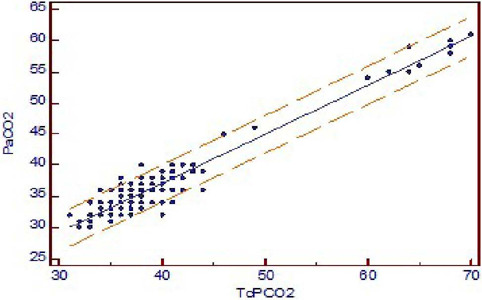
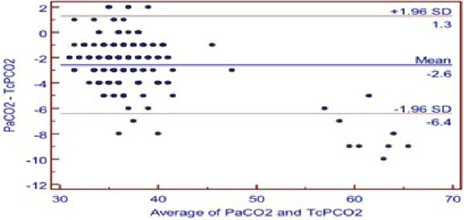
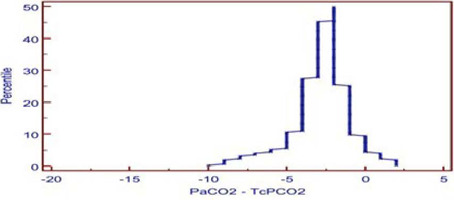
Methods: We conducted a study on 30 pediatric post-cardiac surgery patients (four months to three years old) who were extubated and exhibited stable hemodynamics (inotropic score ≤ 5), normal sinus rhythm, and no respiratory or heart failure signs. Continuous transcutaneous and intermittent arterial blood gas monitoring started one hour after extubation, with recordings every 30 minutes for four hours. A single observer conducted probe calibration and data recording to minimize variability, while analysis of 240 paired samples included correlation coefficient, linear regression, Bland-Altman analysis, and Mountain plot.
Results: The r-value between PaCO2 and TcPCO2 was 0.95, r2-value of 0.9060 (P<0.001). Bland-Altman showed a bias of 2.579, and 95% limits of agreement were -6.4 to 1.3. The r-value between PaO2 and TcPO2 was 0.8942, r2-value of 0.7996 (P<0.001); bias of 20.171 and 95% limit of agreement of -0.5 to 40.9. The Mountain plot revealed a median of 2.57 for PaCO2 vs. TcPCO2 and 20.17 for PaO2 vs. TcPO2.
Conclusion: Transcutaneous carbon dioxide values are interchangeable with arterial PaCO2 in our population study, acting as a surrogate in postoperative pediatric cardiac surgery. Confirmation with arterial blood gases is needed if discrepancies occur.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


