{"title":"长期机械通气重症监护患者膈功能障碍及肺实质改变的超声检测与随访。","authors":"Büşra Pekince, Yeşim Şerife Bayraktar, Jale Bengi Çelik","doi":"10.5578/tt.202501974","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Previous studies have reported that diaphragm atrophy and dysfunction might occur during mechanical ventilation (MV), but the frequency, effect on mortality, underlying causes and functional outcomes of diaphragm and lung parenchymal changes during routine MV have not yet been fully understood.</p><p><strong>Materials and methods: </strong>The lung parenchyma and diaphragm of 50 patients were investigated using ultrasound (USG) on day 1, 5, and 10 of MV therapy.</p><p><strong>Result: </strong>Mean age of the patients was 64.90 ± 15.96 years. Mean MV duration was 90.18 ± 21.09 days. Mean thickening fraction (TFdi) on day 1, 5, and 10 was 40.77 ± 15.42, 39.85 ± 16.85, and 43.57 ± 19.10, respectively. Mean diaphragm amplitude on day 1, 5, and 10 was 1.70 ± 0.74, 1.76 ± 0.74, and 1.70 ± 0.71, respectively. Mean diaphragmatic thickness at the end of expiration (Tde) on day 1, 5, and 10 was 0.18 ± 0.08, 0.17 ± 0.06, and 0.16 ± 0.05, respectively. There was no significant change between measurement days by TFdi, diaphragmatic amplitude (DA), and Tde values. On admission, TFdi was less than 20% in 8% of the patients, DA was less than 1 cm in 12%, and Tfde was less than 0.2 cm in 52%. There was no significant difference by the TFdi, DA and lung ultrasonography (LUS) scores of the non-surviving and surviving patients. An analysis of imaging results and LUS scores indicated that LUS values were measured higher in patients with infiltration on chest radiography. In addition, LUS scores significantly decreased from day 1 to day 5 and day 10, and from day 5 to day 10.</p><p><strong>Conclusions: </strong>Diaphragm dysfunction may occur as a result of MV therapy or associated with an inflammatory process, including sepsis. Assessment of diaphragmatic function by USG on admission to the intensive care unit may help to better recognize and manage diaphragmatic dysfunction. LUS provides information about the lung parenchyma as important as chest X-ray and facilitates bedside patient evaluation.</p>","PeriodicalId":519894,"journal":{"name":"Tuberkuloz ve toraks","volume":"73 1","pages":"1-10"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11977901/pdf/","citationCount":"0","resultStr":"{\"title\":\"Detection and follow-up of diaphragmatic dysfunction and lung parenchymal changes by ultrasound in intensive care patients receiving long-term mechanical ventilation.\",\"authors\":\"Büşra Pekince, Yeşim Şerife Bayraktar, Jale Bengi Çelik\",\"doi\":\"10.5578/tt.202501974\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Previous studies have reported that diaphragm atrophy and dysfunction might occur during mechanical ventilation (MV), but the frequency, effect on mortality, underlying causes and functional outcomes of diaphragm and lung parenchymal changes during routine MV have not yet been fully understood.</p><p><strong>Materials and methods: </strong>The lung parenchyma and diaphragm of 50 patients were investigated using ultrasound (USG) on day 1, 5, and 10 of MV therapy.</p><p><strong>Result: </strong>Mean age of the patients was 64.90 ± 15.96 years. Mean MV duration was 90.18 ± 21.09 days. Mean thickening fraction (TFdi) on day 1, 5, and 10 was 40.77 ± 15.42, 39.85 ± 16.85, and 43.57 ± 19.10, respectively. Mean diaphragm amplitude on day 1, 5, and 10 was 1.70 ± 0.74, 1.76 ± 0.74, and 1.70 ± 0.71, respectively. Mean diaphragmatic thickness at the end of expiration (Tde) on day 1, 5, and 10 was 0.18 ± 0.08, 0.17 ± 0.06, and 0.16 ± 0.05, respectively. There was no significant change between measurement days by TFdi, diaphragmatic amplitude (DA), and Tde values. On admission, TFdi was less than 20% in 8% of the patients, DA was less than 1 cm in 12%, and Tfde was less than 0.2 cm in 52%. There was no significant difference by the TFdi, DA and lung ultrasonography (LUS) scores of the non-surviving and surviving patients. An analysis of imaging results and LUS scores indicated that LUS values were measured higher in patients with infiltration on chest radiography. In addition, LUS scores significantly decreased from day 1 to day 5 and day 10, and from day 5 to day 10.</p><p><strong>Conclusions: </strong>Diaphragm dysfunction may occur as a result of MV therapy or associated with an inflammatory process, including sepsis. Assessment of diaphragmatic function by USG on admission to the intensive care unit may help to better recognize and manage diaphragmatic dysfunction. LUS provides information about the lung parenchyma as important as chest X-ray and facilitates bedside patient evaluation.</p>\",\"PeriodicalId\":519894,\"journal\":{\"name\":\"Tuberkuloz ve toraks\",\"volume\":\"73 1\",\"pages\":\"1-10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11977901/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tuberkuloz ve toraks\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5578/tt.202501974\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tuberkuloz ve toraks","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5578/tt.202501974","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Detection and follow-up of diaphragmatic dysfunction and lung parenchymal changes by ultrasound in intensive care patients receiving long-term mechanical ventilation.
Introduction: Previous studies have reported that diaphragm atrophy and dysfunction might occur during mechanical ventilation (MV), but the frequency, effect on mortality, underlying causes and functional outcomes of diaphragm and lung parenchymal changes during routine MV have not yet been fully understood.
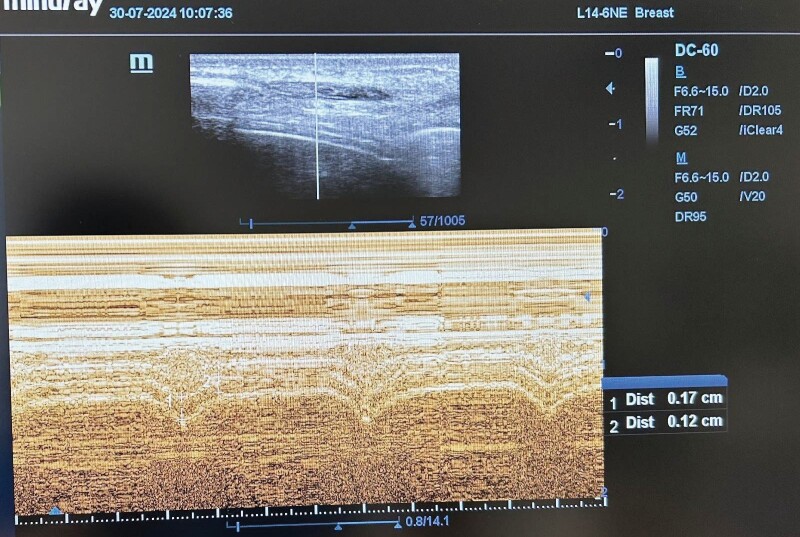
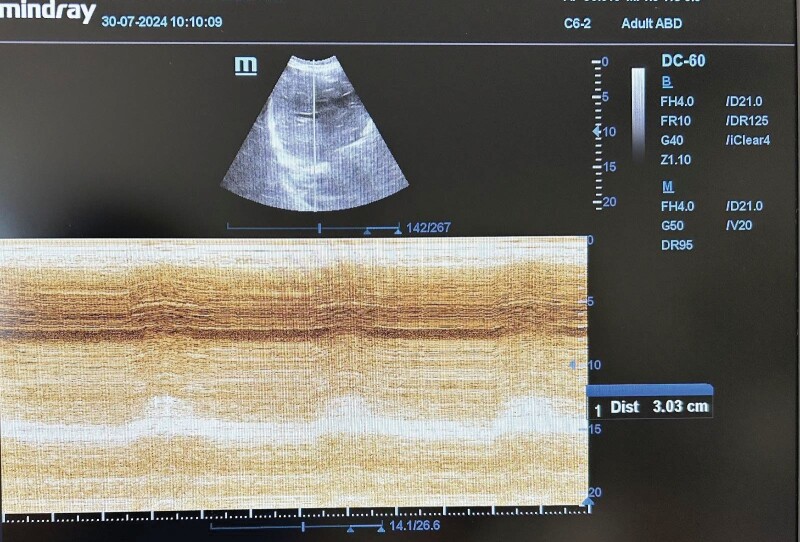
Materials and methods: The lung parenchyma and diaphragm of 50 patients were investigated using ultrasound (USG) on day 1, 5, and 10 of MV therapy.
Result: Mean age of the patients was 64.90 ± 15.96 years. Mean MV duration was 90.18 ± 21.09 days. Mean thickening fraction (TFdi) on day 1, 5, and 10 was 40.77 ± 15.42, 39.85 ± 16.85, and 43.57 ± 19.10, respectively. Mean diaphragm amplitude on day 1, 5, and 10 was 1.70 ± 0.74, 1.76 ± 0.74, and 1.70 ± 0.71, respectively. Mean diaphragmatic thickness at the end of expiration (Tde) on day 1, 5, and 10 was 0.18 ± 0.08, 0.17 ± 0.06, and 0.16 ± 0.05, respectively. There was no significant change between measurement days by TFdi, diaphragmatic amplitude (DA), and Tde values. On admission, TFdi was less than 20% in 8% of the patients, DA was less than 1 cm in 12%, and Tfde was less than 0.2 cm in 52%. There was no significant difference by the TFdi, DA and lung ultrasonography (LUS) scores of the non-surviving and surviving patients. An analysis of imaging results and LUS scores indicated that LUS values were measured higher in patients with infiltration on chest radiography. In addition, LUS scores significantly decreased from day 1 to day 5 and day 10, and from day 5 to day 10.
Conclusions: Diaphragm dysfunction may occur as a result of MV therapy or associated with an inflammatory process, including sepsis. Assessment of diaphragmatic function by USG on admission to the intensive care unit may help to better recognize and manage diaphragmatic dysfunction. LUS provides information about the lung parenchyma as important as chest X-ray and facilitates bedside patient evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


