Kimberly B Golisch, Casey M Silver, Ying Shan, Andres Guerra, Lauren M Janczewski, Jeanette Chung, Brianna D'Orazio, Julie K Johnson, Vivek N Prachand, Michael F McGee, David D Odell, Anthony D Yang, Karl Y Bilimoria, Ryan P Merkow
{"title":"混合方法评价协作范围内的质量改善项目,以改善腹腔盆腔癌手术后静脉血栓栓塞化学预防。","authors":"Kimberly B Golisch, Casey M Silver, Ying Shan, Andres Guerra, Lauren M Janczewski, Jeanette Chung, Brianna D'Orazio, Julie K Johnson, Vivek N Prachand, Michael F McGee, David D Odell, Anthony D Yang, Karl Y Bilimoria, Ryan P Merkow","doi":"10.1097/AS9.0000000000000555","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We studied a collaborative-wide quality improvement project (CQIP) focused on improving postdischarge venous thromboembolism (VTE) chemoprophylaxis adherence. We aimed to identify patient-level characteristics associated with adherence, evaluate differences in adherence rates among participating hospitals, and assess facilitators and barriers to adherence at high- and low-performing hospitals.</p><p><strong>Background: </strong>VTE is the most common preventable cause of death after abdominopelvic cancer surgery, yet adherence to guideline-recommended postdischarge VTE chemoprophylaxis remains suboptimal. A CQIP including audit and feedback of performance data, a toolkit, coaching calls, and best practice alerts was implemented.</p><p><strong>Methods: </strong>Patients undergoing inpatient abdominopelvic cancer surgery at a CQIP-enrolled hospital during a 3-year study period were included. Unadjusted and adjusted rates were calculated for postdischarge VTE chemoprophylaxis adherence. High performance was defined as >10% improvement and/or ≥80% adherence. We conducted semistructured interviews and focus groups with collaborative members to identify barriers and facilitators to implementation.</p><p><strong>Results: </strong>Postdischarge VTE chemoprophylaxis adherence increased from 51.8% (preimplementation) to 64.5% (postimplementation; <i>P</i> < 0.05). Patients who underwent urologic (odds ratio [OR], 1.76 [95% CI, 1.27-2.43]) and gynecologic procedures (OR, 3.90 [95% CI, 2.73-5.58]) were more likely prescribed appropriate VTE chemoprophylaxis compared with colorectal procedures. Eight hospitals (50%) had improvement in adherence rates, and 8 (50%) were high performers. Barriers to implementation included a lack of surgeon buy-in, technical challenges, and a lack of awareness.</p><p><strong>Conclusions: </strong>A CQIP was associated with increased postdischarge VTE adherence rates. Different barriers exist between high- and low-performing hospitals. Future collaborative work should focus on hospital-level interventions to improve low-performer results.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"6 1","pages":"e555"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932594/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Mixed-Methods Evaluation of a Collaborative-Wide Quality Improvement Project to Improve Postdischarge Venous Thromboembolism Chemoprophylaxis After Abdominopelvic Cancer Surgery.\",\"authors\":\"Kimberly B Golisch, Casey M Silver, Ying Shan, Andres Guerra, Lauren M Janczewski, Jeanette Chung, Brianna D'Orazio, Julie K Johnson, Vivek N Prachand, Michael F McGee, David D Odell, Anthony D Yang, Karl Y Bilimoria, Ryan P Merkow\",\"doi\":\"10.1097/AS9.0000000000000555\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We studied a collaborative-wide quality improvement project (CQIP) focused on improving postdischarge venous thromboembolism (VTE) chemoprophylaxis adherence. We aimed to identify patient-level characteristics associated with adherence, evaluate differences in adherence rates among participating hospitals, and assess facilitators and barriers to adherence at high- and low-performing hospitals.</p><p><strong>Background: </strong>VTE is the most common preventable cause of death after abdominopelvic cancer surgery, yet adherence to guideline-recommended postdischarge VTE chemoprophylaxis remains suboptimal. A CQIP including audit and feedback of performance data, a toolkit, coaching calls, and best practice alerts was implemented.</p><p><strong>Methods: </strong>Patients undergoing inpatient abdominopelvic cancer surgery at a CQIP-enrolled hospital during a 3-year study period were included. Unadjusted and adjusted rates were calculated for postdischarge VTE chemoprophylaxis adherence. High performance was defined as >10% improvement and/or ≥80% adherence. We conducted semistructured interviews and focus groups with collaborative members to identify barriers and facilitators to implementation.</p><p><strong>Results: </strong>Postdischarge VTE chemoprophylaxis adherence increased from 51.8% (preimplementation) to 64.5% (postimplementation; <i>P</i> < 0.05). Patients who underwent urologic (odds ratio [OR], 1.76 [95% CI, 1.27-2.43]) and gynecologic procedures (OR, 3.90 [95% CI, 2.73-5.58]) were more likely prescribed appropriate VTE chemoprophylaxis compared with colorectal procedures. Eight hospitals (50%) had improvement in adherence rates, and 8 (50%) were high performers. Barriers to implementation included a lack of surgeon buy-in, technical challenges, and a lack of awareness.</p><p><strong>Conclusions: </strong>A CQIP was associated with increased postdischarge VTE adherence rates. Different barriers exist between high- and low-performing hospitals. Future collaborative work should focus on hospital-level interventions to improve low-performer results.</p>\",\"PeriodicalId\":72231,\"journal\":{\"name\":\"Annals of surgery open : perspectives of surgical history, education, and clinical approaches\",\"volume\":\"6 1\",\"pages\":\"e555\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932594/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of surgery open : perspectives of surgical history, education, and clinical approaches\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/AS9.0000000000000555\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000555","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A Mixed-Methods Evaluation of a Collaborative-Wide Quality Improvement Project to Improve Postdischarge Venous Thromboembolism Chemoprophylaxis After Abdominopelvic Cancer Surgery.
Objective: We studied a collaborative-wide quality improvement project (CQIP) focused on improving postdischarge venous thromboembolism (VTE) chemoprophylaxis adherence. We aimed to identify patient-level characteristics associated with adherence, evaluate differences in adherence rates among participating hospitals, and assess facilitators and barriers to adherence at high- and low-performing hospitals.
Background: VTE is the most common preventable cause of death after abdominopelvic cancer surgery, yet adherence to guideline-recommended postdischarge VTE chemoprophylaxis remains suboptimal. A CQIP including audit and feedback of performance data, a toolkit, coaching calls, and best practice alerts was implemented.
Methods: Patients undergoing inpatient abdominopelvic cancer surgery at a CQIP-enrolled hospital during a 3-year study period were included. Unadjusted and adjusted rates were calculated for postdischarge VTE chemoprophylaxis adherence. High performance was defined as >10% improvement and/or ≥80% adherence. We conducted semistructured interviews and focus groups with collaborative members to identify barriers and facilitators to implementation.
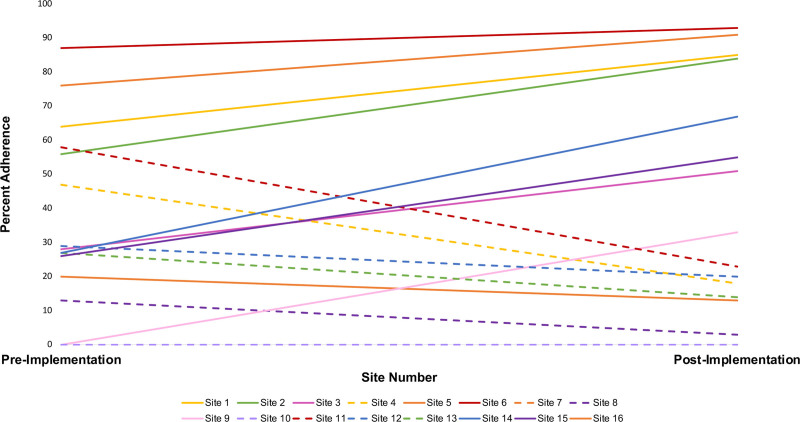
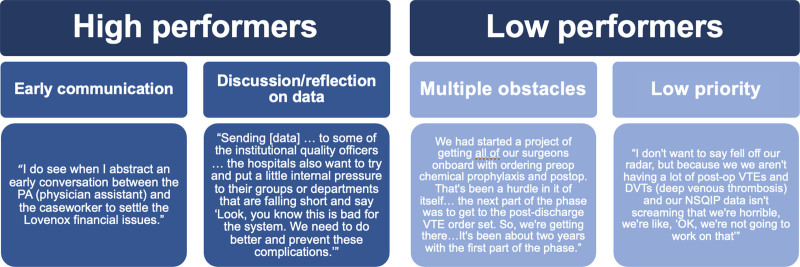
Results: Postdischarge VTE chemoprophylaxis adherence increased from 51.8% (preimplementation) to 64.5% (postimplementation; P < 0.05). Patients who underwent urologic (odds ratio [OR], 1.76 [95% CI, 1.27-2.43]) and gynecologic procedures (OR, 3.90 [95% CI, 2.73-5.58]) were more likely prescribed appropriate VTE chemoprophylaxis compared with colorectal procedures. Eight hospitals (50%) had improvement in adherence rates, and 8 (50%) were high performers. Barriers to implementation included a lack of surgeon buy-in, technical challenges, and a lack of awareness.
Conclusions: A CQIP was associated with increased postdischarge VTE adherence rates. Different barriers exist between high- and low-performing hospitals. Future collaborative work should focus on hospital-level interventions to improve low-performer results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


