Cody Lendon Mullens, Sarah Sheskey, Edward C Norton, Jyothi R Thumma, Hari Nathan, Scott E Regenbogen, Kyle H Sheetz
{"title":"使用工具变量分析的结直肠癌手术入路和术后长期生存的变化。","authors":"Cody Lendon Mullens, Sarah Sheskey, Edward C Norton, Jyothi R Thumma, Hari Nathan, Scott E Regenbogen, Kyle H Sheetz","doi":"10.1097/AS9.0000000000000538","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study aimed to determine whether increased use of minimally invasive surgical approaches, compared with open, improves long-term survival after colon and rectal cancer resections.</p><p><strong>Background: </strong>Existing prospective and observational data comparing surgical approach for colon and rectal cancer are limited by selection bias, necessitating better approaches for causal inference to understand the relationship between surgical approach and long-term survival.</p><p><strong>Methods: </strong>We included colon and rectal cancer patients who underwent colon or rectal resection from the American College of Surgeons National Cancer Database between 2011 and 2018. Using an instrumental variable (IV) approach, we accounted for measured and unmeasured differences between patients undergoing colon or rectal cancer resection based on operative approach - robotic, laparoscopic, or open. The IV used in this study was rate of robotic-assisted colon and rectal cancer surgery within 81 different hospital regions based on US Census region and rurality during the 12 months before each patient's operation. Proportional hazard modeling was used to estimate risk-adjusted mortality rates.</p><p><strong>Results: </strong>There were 326,406 colon and 96,979 rectal cancer patients included in this study. The risk-adjusted 5-year cumulative incidence of mortality for colon and rectal cancer was highest for patients who underwent open approaches (35.73 [95% confidence interval {CI}: 35.37-36.1] and 39.27 [95% CI: 28.44-30.13], respectively), compared with lower mortality for those undergoing laparoscopic (28.91 [95% CI: 28.55-29.27] and 22.93 [95% CI: 22.11-23.78], respectively) and robotic approaches (26.39 [95% CI: 24.51-28.42] and 19.77 [95% CI: 17.32-22.43], respectively). Growth in utilization of minimally invasive approaches outpaced improvements in long-term survival.</p><p><strong>Conclusions: </strong>Patients undergoing minimally invasive surgical approaches for colon and rectal cancer had improved long-term survival. However, long-term survival changes did not correlate with the large expansion of minimally invasive approaches, which suggests that growing these approaches is not a viable strategy to improve long-term patient outcomes.</p>","PeriodicalId":72231,"journal":{"name":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","volume":"6 1","pages":"e538"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932609/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical Approach and Variation in Long-Term Survival Following Colorectal Cancer Surgery Using Instrumental Variable Analysis.\",\"authors\":\"Cody Lendon Mullens, Sarah Sheskey, Edward C Norton, Jyothi R Thumma, Hari Nathan, Scott E Regenbogen, Kyle H Sheetz\",\"doi\":\"10.1097/AS9.0000000000000538\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The study aimed to determine whether increased use of minimally invasive surgical approaches, compared with open, improves long-term survival after colon and rectal cancer resections.</p><p><strong>Background: </strong>Existing prospective and observational data comparing surgical approach for colon and rectal cancer are limited by selection bias, necessitating better approaches for causal inference to understand the relationship between surgical approach and long-term survival.</p><p><strong>Methods: </strong>We included colon and rectal cancer patients who underwent colon or rectal resection from the American College of Surgeons National Cancer Database between 2011 and 2018. Using an instrumental variable (IV) approach, we accounted for measured and unmeasured differences between patients undergoing colon or rectal cancer resection based on operative approach - robotic, laparoscopic, or open. The IV used in this study was rate of robotic-assisted colon and rectal cancer surgery within 81 different hospital regions based on US Census region and rurality during the 12 months before each patient's operation. Proportional hazard modeling was used to estimate risk-adjusted mortality rates.</p><p><strong>Results: </strong>There were 326,406 colon and 96,979 rectal cancer patients included in this study. The risk-adjusted 5-year cumulative incidence of mortality for colon and rectal cancer was highest for patients who underwent open approaches (35.73 [95% confidence interval {CI}: 35.37-36.1] and 39.27 [95% CI: 28.44-30.13], respectively), compared with lower mortality for those undergoing laparoscopic (28.91 [95% CI: 28.55-29.27] and 22.93 [95% CI: 22.11-23.78], respectively) and robotic approaches (26.39 [95% CI: 24.51-28.42] and 19.77 [95% CI: 17.32-22.43], respectively). Growth in utilization of minimally invasive approaches outpaced improvements in long-term survival.</p><p><strong>Conclusions: </strong>Patients undergoing minimally invasive surgical approaches for colon and rectal cancer had improved long-term survival. However, long-term survival changes did not correlate with the large expansion of minimally invasive approaches, which suggests that growing these approaches is not a viable strategy to improve long-term patient outcomes.</p>\",\"PeriodicalId\":72231,\"journal\":{\"name\":\"Annals of surgery open : perspectives of surgical history, education, and clinical approaches\",\"volume\":\"6 1\",\"pages\":\"e538\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11932609/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of surgery open : perspectives of surgical history, education, and clinical approaches\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/AS9.0000000000000538\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of surgery open : perspectives of surgical history, education, and clinical approaches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/AS9.0000000000000538","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Surgical Approach and Variation in Long-Term Survival Following Colorectal Cancer Surgery Using Instrumental Variable Analysis.
Objective: The study aimed to determine whether increased use of minimally invasive surgical approaches, compared with open, improves long-term survival after colon and rectal cancer resections.
Background: Existing prospective and observational data comparing surgical approach for colon and rectal cancer are limited by selection bias, necessitating better approaches for causal inference to understand the relationship between surgical approach and long-term survival.
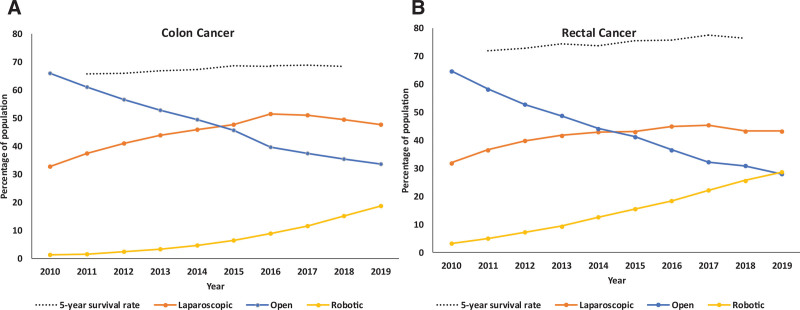
Methods: We included colon and rectal cancer patients who underwent colon or rectal resection from the American College of Surgeons National Cancer Database between 2011 and 2018. Using an instrumental variable (IV) approach, we accounted for measured and unmeasured differences between patients undergoing colon or rectal cancer resection based on operative approach - robotic, laparoscopic, or open. The IV used in this study was rate of robotic-assisted colon and rectal cancer surgery within 81 different hospital regions based on US Census region and rurality during the 12 months before each patient's operation. Proportional hazard modeling was used to estimate risk-adjusted mortality rates.
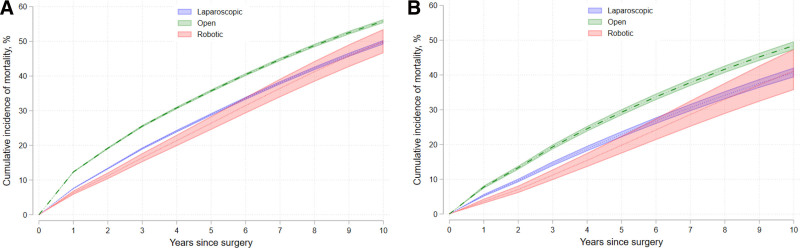
Results: There were 326,406 colon and 96,979 rectal cancer patients included in this study. The risk-adjusted 5-year cumulative incidence of mortality for colon and rectal cancer was highest for patients who underwent open approaches (35.73 [95% confidence interval {CI}: 35.37-36.1] and 39.27 [95% CI: 28.44-30.13], respectively), compared with lower mortality for those undergoing laparoscopic (28.91 [95% CI: 28.55-29.27] and 22.93 [95% CI: 22.11-23.78], respectively) and robotic approaches (26.39 [95% CI: 24.51-28.42] and 19.77 [95% CI: 17.32-22.43], respectively). Growth in utilization of minimally invasive approaches outpaced improvements in long-term survival.
Conclusions: Patients undergoing minimally invasive surgical approaches for colon and rectal cancer had improved long-term survival. However, long-term survival changes did not correlate with the large expansion of minimally invasive approaches, which suggests that growing these approaches is not a viable strategy to improve long-term patient outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


