Karl Teurneau-Hermansson, David von Rosen, Jacob Ede, Mårten Larsson, Johan Sjögren, Per Wierup, Shahab Nozohoor, Igor Zindovic
{"title":"急性A型主动脉夹层初误诊的原因及临床影响。","authors":"Karl Teurneau-Hermansson, David von Rosen, Jacob Ede, Mårten Larsson, Johan Sjögren, Per Wierup, Shahab Nozohoor, Igor Zindovic","doi":"10.1093/ehjopen/oeaf027","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The high mortality in untreated acute type A aortic dissection (ATAAD) stresses the need for prompt diagnosis and immediate surgical treatment. Our aim was to evaluate the frequency and clinical impact of misdiagnosis and delayed diagnosis of ATAAD.</p><p><strong>Methods and results: </strong>This was a single-centre, retrospective, observational study including all ATAAD patients with available admission charts between 2001 and 2021 in an area of 1.9 million inhabitants in southern Sweden. The primary endpoints were initial misdiagnosis, delayed diagnosis, and 30-day mortality. Surgical treatment was a secondary endpoint. Independent predictors of misdiagnosis and 30-day mortality were identified by multivariable logistic regression and subgroup analyses by severity of clinical presentation were performed. There were 556 patients included in the study (418 surgically treated and 138 non-surgically treated), and 45.3% were initially misdiagnosed. Misdiagnosed patients were more often female (47.6 vs. 35.9%; <i>P</i> = 0.005) and demonstrated significantly lower rates of syncope, hypotensive shock, and malperfusion. Patients without signs of malperfusion subjected to diagnostic delay were less likely offered surgical treatment (74.0 vs. 91.5%; <i>P</i> < 0.001) and had higher 30-day mortality (21.3 vs. 10.8%; <i>P</i> = 0.040). Female sex was an independent predictor of misdiagnosis (OR: 1.748; 95% CI 1.145-2.668; <i>P</i> = 0.010), but neither misdiagnosis nor delayed diagnosis were independent predictors of 30-day mortality.</p><p><strong>Conclusion: </strong>Although misdiagnosis and delayed diagnosis did not influence overall 30-day mortality, delayed diagnosis led to significantly higher 30-day mortality in the large group of patients presenting without signs of malperfusion, likely caused by the observed higher risk of being denied surgical treatment.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"5 2","pages":"oeaf027"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11935741/pdf/","citationCount":"0","resultStr":"{\"title\":\"Causes and clinical impact of initial misdiagnosis of acute type A aortic dissection.\",\"authors\":\"Karl Teurneau-Hermansson, David von Rosen, Jacob Ede, Mårten Larsson, Johan Sjögren, Per Wierup, Shahab Nozohoor, Igor Zindovic\",\"doi\":\"10.1093/ehjopen/oeaf027\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The high mortality in untreated acute type A aortic dissection (ATAAD) stresses the need for prompt diagnosis and immediate surgical treatment. Our aim was to evaluate the frequency and clinical impact of misdiagnosis and delayed diagnosis of ATAAD.</p><p><strong>Methods and results: </strong>This was a single-centre, retrospective, observational study including all ATAAD patients with available admission charts between 2001 and 2021 in an area of 1.9 million inhabitants in southern Sweden. The primary endpoints were initial misdiagnosis, delayed diagnosis, and 30-day mortality. Surgical treatment was a secondary endpoint. Independent predictors of misdiagnosis and 30-day mortality were identified by multivariable logistic regression and subgroup analyses by severity of clinical presentation were performed. There were 556 patients included in the study (418 surgically treated and 138 non-surgically treated), and 45.3% were initially misdiagnosed. Misdiagnosed patients were more often female (47.6 vs. 35.9%; <i>P</i> = 0.005) and demonstrated significantly lower rates of syncope, hypotensive shock, and malperfusion. Patients without signs of malperfusion subjected to diagnostic delay were less likely offered surgical treatment (74.0 vs. 91.5%; <i>P</i> < 0.001) and had higher 30-day mortality (21.3 vs. 10.8%; <i>P</i> = 0.040). Female sex was an independent predictor of misdiagnosis (OR: 1.748; 95% CI 1.145-2.668; <i>P</i> = 0.010), but neither misdiagnosis nor delayed diagnosis were independent predictors of 30-day mortality.</p><p><strong>Conclusion: </strong>Although misdiagnosis and delayed diagnosis did not influence overall 30-day mortality, delayed diagnosis led to significantly higher 30-day mortality in the large group of patients presenting without signs of malperfusion, likely caused by the observed higher risk of being denied surgical treatment.</p>\",\"PeriodicalId\":93995,\"journal\":{\"name\":\"European heart journal open\",\"volume\":\"5 2\",\"pages\":\"oeaf027\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11935741/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjopen/oeaf027\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oeaf027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:急性A型主动脉夹层(ATAAD)未经治疗的高死亡率强调了及时诊断和立即手术治疗的必要性。我们的目的是评估误诊和延迟诊断ATAAD的频率和临床影响。方法和结果:这是一项单中心、回顾性、观察性研究,纳入了瑞典南部190万居民中2001年至2021年间所有可获得入院表的ATAAD患者。主要终点为初始误诊、延迟诊断和30天死亡率。手术治疗是次要终点。通过多变量logistic回归确定误诊和30天死亡率的独立预测因子,并根据临床表现的严重程度进行亚组分析。共纳入556例患者(手术治疗418例,非手术治疗138例),45.3%的患者最初被误诊。误诊患者多为女性(47.6% vs. 35.9%;P = 0.005),晕厥、低血压性休克和灌注不良的发生率明显降低。无灌注不良症状的患者诊断延迟接受手术治疗的可能性较小(74.0比91.5%;P < 0.001),且30天死亡率更高(21.3%比10.8%;P = 0.040)。女性是误诊的独立预测因子(OR: 1.748;95% ci 1.145-2.668;P = 0.010),但误诊和延迟诊断都不是30天死亡率的独立预测因素。结论:虽然误诊和延迟诊断不影响总体30天死亡率,但延迟诊断导致大量无灌注不良体征患者的30天死亡率显著升高,这可能是由于观察到被拒绝手术治疗的风险较高。
Causes and clinical impact of initial misdiagnosis of acute type A aortic dissection.
Aims: The high mortality in untreated acute type A aortic dissection (ATAAD) stresses the need for prompt diagnosis and immediate surgical treatment. Our aim was to evaluate the frequency and clinical impact of misdiagnosis and delayed diagnosis of ATAAD.
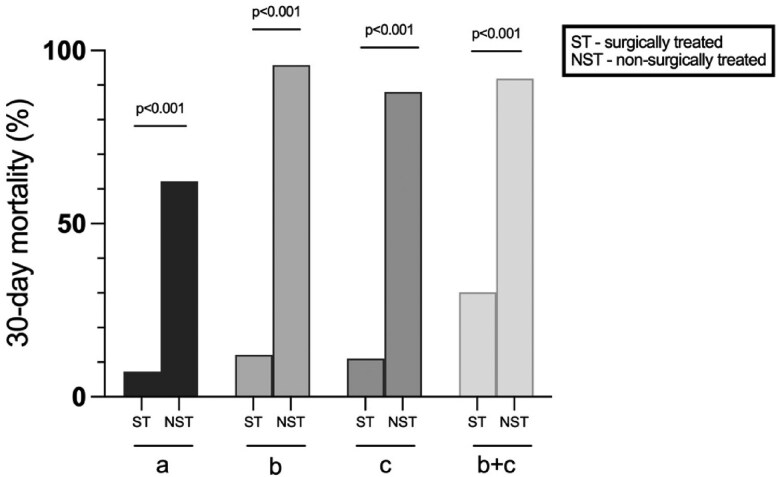
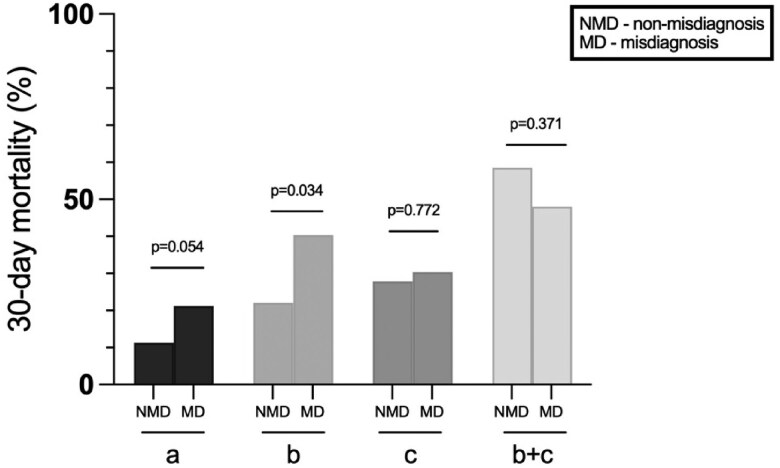
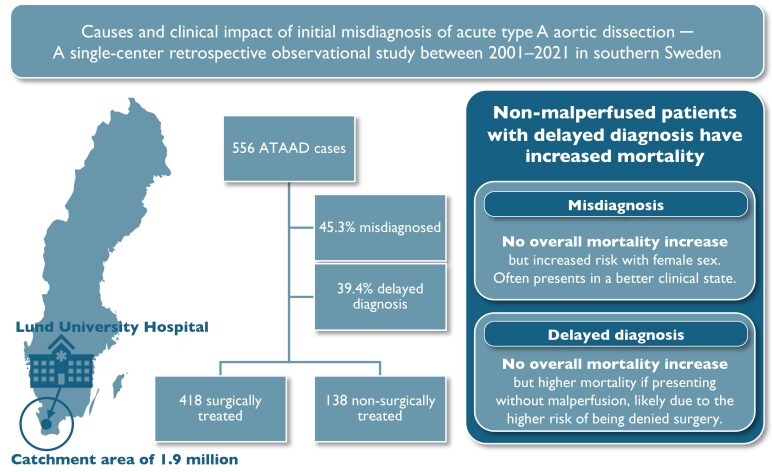
Methods and results: This was a single-centre, retrospective, observational study including all ATAAD patients with available admission charts between 2001 and 2021 in an area of 1.9 million inhabitants in southern Sweden. The primary endpoints were initial misdiagnosis, delayed diagnosis, and 30-day mortality. Surgical treatment was a secondary endpoint. Independent predictors of misdiagnosis and 30-day mortality were identified by multivariable logistic regression and subgroup analyses by severity of clinical presentation were performed. There were 556 patients included in the study (418 surgically treated and 138 non-surgically treated), and 45.3% were initially misdiagnosed. Misdiagnosed patients were more often female (47.6 vs. 35.9%; P = 0.005) and demonstrated significantly lower rates of syncope, hypotensive shock, and malperfusion. Patients without signs of malperfusion subjected to diagnostic delay were less likely offered surgical treatment (74.0 vs. 91.5%; P < 0.001) and had higher 30-day mortality (21.3 vs. 10.8%; P = 0.040). Female sex was an independent predictor of misdiagnosis (OR: 1.748; 95% CI 1.145-2.668; P = 0.010), but neither misdiagnosis nor delayed diagnosis were independent predictors of 30-day mortality.
Conclusion: Although misdiagnosis and delayed diagnosis did not influence overall 30-day mortality, delayed diagnosis led to significantly higher 30-day mortality in the large group of patients presenting without signs of malperfusion, likely caused by the observed higher risk of being denied surgical treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


