Peter Murin, Julia Gaal, Robin Stenzel, Viktoria Weixler, Olga Romanchenko, Raphael Seiler, Stanislav Ovroutski, Felix Berger, Mi-Young Cho, Joachim Photiadis, Marcus Kelm
{"title":"儿童ross手术的最佳结果:单中心经验。","authors":"Peter Murin, Julia Gaal, Robin Stenzel, Viktoria Weixler, Olga Romanchenko, Raphael Seiler, Stanislav Ovroutski, Felix Berger, Mi-Young Cho, Joachim Photiadis, Marcus Kelm","doi":"10.1093/ejcts/ezaf102","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The Ross procedure with autograft reinforcement has been proposed as a strategy to prevent autograft failure in adults, but outcome data in children during somatic growth remain limited. We investigated long-term outcomes following an individualized autograft reinforcement protocol to evaluate survival and reintervention rates.</p><p><strong>Methods: </strong>Between January 1995 and December 2022, 233 patients <18 years [median age: 7 (1-13) years] underwent the Ross procedure, including 60 infants (26%). Most frequently free-root autograft implantation without reinforcement was performed (n = 156, 67%). Autograft reinforcement was applied in 77 patients (33%) using either subcoronary implantation (n = 65, 28%) or external prosthetic support (n = 12, 5%). Kaplan-Meier survival estimates were used for survival and reintervention analyses. Risk factors for reintervention were identified by Cox proportional hazards regression.</p><p><strong>Results: </strong>Reinforcement was associated with improved survival (5-year survival rates of 97.1% vs 87.0%, 10-year survival rates of 97.1% versus 86.99%, P = 0.017). No differences in autograft reintervention between the groups were found (1-year rates of 100% vs 99.4%, 5-year rates of 100%, P = 0.4852). Right ventricle-pulmonary artery (RV-PA) reintervention-free survival at 5 years was higher for homografts compared to xenografts (96.9% vs 79.4%, P < 0.001).</p><p><strong>Conclusions: </strong>The Ross procedure in children demonstrated excellent long-term outcomes with low autograft reintervention rates in both groups. Reinforcement was associated with improved long-term survival while autograft-related reinterventions did not differ significantly between groups. Older age at Ross and homograft use correlated with lower RV-PA reintervention risk. Multicentre evaluation of reinforcement techniques is required to assess the outcome differences observed in this single-centre experience.</p>","PeriodicalId":11938,"journal":{"name":"European Journal of Cardio-Thoracic Surgery","volume":" ","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-03-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11992329/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimized outcome of the Ross procedure in children: single-centre experience†.\",\"authors\":\"Peter Murin, Julia Gaal, Robin Stenzel, Viktoria Weixler, Olga Romanchenko, Raphael Seiler, Stanislav Ovroutski, Felix Berger, Mi-Young Cho, Joachim Photiadis, Marcus Kelm\",\"doi\":\"10.1093/ejcts/ezaf102\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The Ross procedure with autograft reinforcement has been proposed as a strategy to prevent autograft failure in adults, but outcome data in children during somatic growth remain limited. We investigated long-term outcomes following an individualized autograft reinforcement protocol to evaluate survival and reintervention rates.</p><p><strong>Methods: </strong>Between January 1995 and December 2022, 233 patients <18 years [median age: 7 (1-13) years] underwent the Ross procedure, including 60 infants (26%). Most frequently free-root autograft implantation without reinforcement was performed (n = 156, 67%). Autograft reinforcement was applied in 77 patients (33%) using either subcoronary implantation (n = 65, 28%) or external prosthetic support (n = 12, 5%). Kaplan-Meier survival estimates were used for survival and reintervention analyses. Risk factors for reintervention were identified by Cox proportional hazards regression.</p><p><strong>Results: </strong>Reinforcement was associated with improved survival (5-year survival rates of 97.1% vs 87.0%, 10-year survival rates of 97.1% versus 86.99%, P = 0.017). No differences in autograft reintervention between the groups were found (1-year rates of 100% vs 99.4%, 5-year rates of 100%, P = 0.4852). Right ventricle-pulmonary artery (RV-PA) reintervention-free survival at 5 years was higher for homografts compared to xenografts (96.9% vs 79.4%, P < 0.001).</p><p><strong>Conclusions: </strong>The Ross procedure in children demonstrated excellent long-term outcomes with low autograft reintervention rates in both groups. Reinforcement was associated with improved long-term survival while autograft-related reinterventions did not differ significantly between groups. Older age at Ross and homograft use correlated with lower RV-PA reintervention risk. Multicentre evaluation of reinforcement techniques is required to assess the outcome differences observed in this single-centre experience.</p>\",\"PeriodicalId\":11938,\"journal\":{\"name\":\"European Journal of Cardio-Thoracic Surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-03-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11992329/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Cardio-Thoracic Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ejcts/ezaf102\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Cardio-Thoracic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ejcts/ezaf102","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:自体移植物加固的Ross手术已被提出作为预防成人自体移植物失败的策略,但在儿童体生长期间的结果数据仍然有限。我们调查了个体化自体移植物加固方案后的长期结果,以评估生存率和再干预率。方法:1995年1月至2022年12月,共233例患者。结果:强化治疗与生存率提高相关(5年生存率为97.1%对87.0%,10年生存率为97.1%对86.99%,p = 0.017)。两组间自体移植物再干预率无差异(1年为100% vs 99.4%, 5年为100%,p = 0.4852)。同种移植物的5年无RV-PA再干预生存率高于异种移植物(96.9% vs 79.4%)。结论:Ross手术在儿童中表现出良好的长期疗效,两组自体移植物再干预率均较低。强化与改善长期生存相关,而自体移植物相关的再干预在两组之间没有显著差异。年龄较大的Ross患者和同种移植物患者再干预风险较低。需要对强化技术进行多中心评估,以评估在单中心经验中观察到的结果差异。
Optimized outcome of the Ross procedure in children: single-centre experience†.
Objectives: The Ross procedure with autograft reinforcement has been proposed as a strategy to prevent autograft failure in adults, but outcome data in children during somatic growth remain limited. We investigated long-term outcomes following an individualized autograft reinforcement protocol to evaluate survival and reintervention rates.
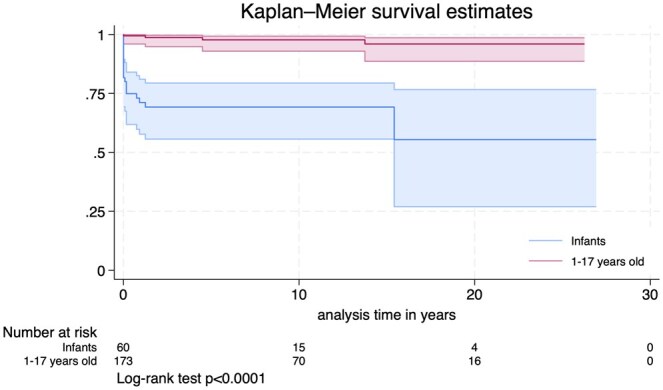
Methods: Between January 1995 and December 2022, 233 patients <18 years [median age: 7 (1-13) years] underwent the Ross procedure, including 60 infants (26%). Most frequently free-root autograft implantation without reinforcement was performed (n = 156, 67%). Autograft reinforcement was applied in 77 patients (33%) using either subcoronary implantation (n = 65, 28%) or external prosthetic support (n = 12, 5%). Kaplan-Meier survival estimates were used for survival and reintervention analyses. Risk factors for reintervention were identified by Cox proportional hazards regression.
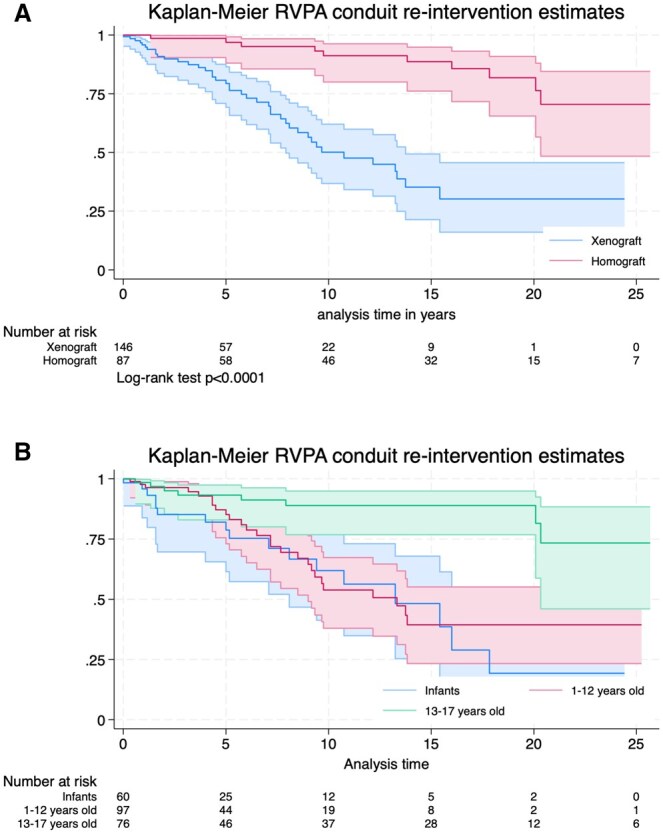
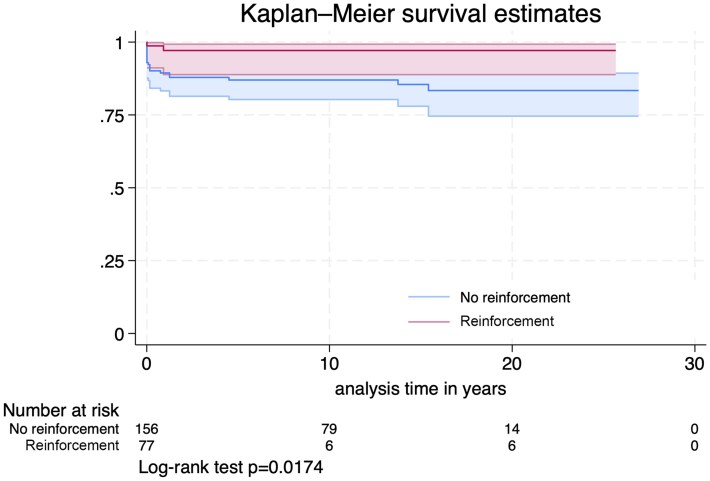
Results: Reinforcement was associated with improved survival (5-year survival rates of 97.1% vs 87.0%, 10-year survival rates of 97.1% versus 86.99%, P = 0.017). No differences in autograft reintervention between the groups were found (1-year rates of 100% vs 99.4%, 5-year rates of 100%, P = 0.4852). Right ventricle-pulmonary artery (RV-PA) reintervention-free survival at 5 years was higher for homografts compared to xenografts (96.9% vs 79.4%, P < 0.001).
Conclusions: The Ross procedure in children demonstrated excellent long-term outcomes with low autograft reintervention rates in both groups. Reinforcement was associated with improved long-term survival while autograft-related reinterventions did not differ significantly between groups. Older age at Ross and homograft use correlated with lower RV-PA reintervention risk. Multicentre evaluation of reinforcement techniques is required to assess the outcome differences observed in this single-centre experience.
期刊介绍:
The primary aim of the European Journal of Cardio-Thoracic Surgery is to provide a medium for the publication of high-quality original scientific reports documenting progress in cardiac and thoracic surgery. The journal publishes reports of significant clinical and experimental advances related to surgery of the heart, the great vessels and the chest. The European Journal of Cardio-Thoracic Surgery is an international journal and accepts submissions from all regions. The journal is supported by a number of leading European societies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


