Aldo Bonaventura, Davide Santagata, Alessandra Vecchié, Antonio Abbate
{"title":"急性和复发性心包炎的药物治疗现状。","authors":"Aldo Bonaventura, Davide Santagata, Alessandra Vecchié, Antonio Abbate","doi":"10.1007/s40265-025-02169-x","DOIUrl":null,"url":null,"abstract":"<p><p>Pericarditis is the most frequent pericardial disease and presents with a relatively benign course when treated according to guideline-directed therapies at first presentation. Recurrence is the most frequent complication and may occur more frequently after a first episode, in patients with autoimmune etiology, in patients who received glucocorticoids, or after rapid (i.e., within 1 month) tapering of anti-inflammatory drugs. The therapeutic armamentarium for pericarditis includes high-dose nonsteroidal anti-inflammatory drugs (NSAIDs) that are tapered rapidly once symptoms are controlled. Colchicine is necessary to both relieve symptoms and reduce the rate of recurrences and is continued for at least 3-6 months. Low- to moderate-dose glucocorticoids are reserved for patients with a first recurrence for which NSAIDs and colchicine failed and/or who have an autoimmune disorder, with a slow tapering. Interleukin-1 blockers-anakinra, rilonacept, and goflikicept-are used as a third-line option in patients who cannot come off glucocorticoids or as second-line therapy after NSAIDs and colchicine in patients with contraindications to glucocorticoids or in those with high-risk features (i.e., multiple episodes, markedly elevated inflammatory markers, or extensive abnormalities at pericardial imaging) in whom treatment with glucocorticoids is unlikely to succeed.</p>","PeriodicalId":11482,"journal":{"name":"Drugs","volume":" ","pages":"643-658"},"PeriodicalIF":14.4000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12031812/pdf/","citationCount":"0","resultStr":"{\"title\":\"Current Drug Treatment for Acute and Recurrent Pericarditis.\",\"authors\":\"Aldo Bonaventura, Davide Santagata, Alessandra Vecchié, Antonio Abbate\",\"doi\":\"10.1007/s40265-025-02169-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Pericarditis is the most frequent pericardial disease and presents with a relatively benign course when treated according to guideline-directed therapies at first presentation. Recurrence is the most frequent complication and may occur more frequently after a first episode, in patients with autoimmune etiology, in patients who received glucocorticoids, or after rapid (i.e., within 1 month) tapering of anti-inflammatory drugs. The therapeutic armamentarium for pericarditis includes high-dose nonsteroidal anti-inflammatory drugs (NSAIDs) that are tapered rapidly once symptoms are controlled. Colchicine is necessary to both relieve symptoms and reduce the rate of recurrences and is continued for at least 3-6 months. Low- to moderate-dose glucocorticoids are reserved for patients with a first recurrence for which NSAIDs and colchicine failed and/or who have an autoimmune disorder, with a slow tapering. Interleukin-1 blockers-anakinra, rilonacept, and goflikicept-are used as a third-line option in patients who cannot come off glucocorticoids or as second-line therapy after NSAIDs and colchicine in patients with contraindications to glucocorticoids or in those with high-risk features (i.e., multiple episodes, markedly elevated inflammatory markers, or extensive abnormalities at pericardial imaging) in whom treatment with glucocorticoids is unlikely to succeed.</p>\",\"PeriodicalId\":11482,\"journal\":{\"name\":\"Drugs\",\"volume\":\" \",\"pages\":\"643-658\"},\"PeriodicalIF\":14.4000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12031812/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40265-025-02169-x\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40265-025-02169-x","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Current Drug Treatment for Acute and Recurrent Pericarditis.
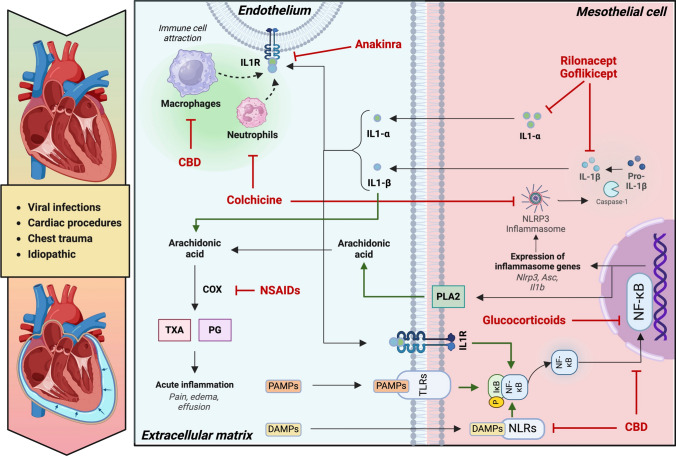
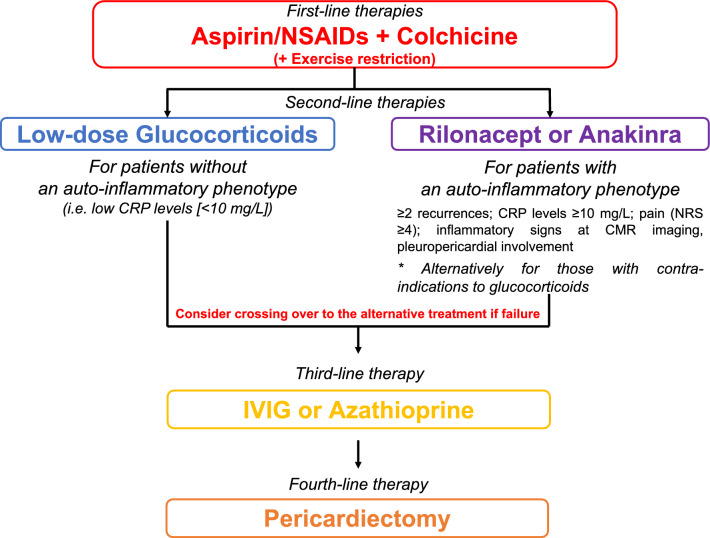
Pericarditis is the most frequent pericardial disease and presents with a relatively benign course when treated according to guideline-directed therapies at first presentation. Recurrence is the most frequent complication and may occur more frequently after a first episode, in patients with autoimmune etiology, in patients who received glucocorticoids, or after rapid (i.e., within 1 month) tapering of anti-inflammatory drugs. The therapeutic armamentarium for pericarditis includes high-dose nonsteroidal anti-inflammatory drugs (NSAIDs) that are tapered rapidly once symptoms are controlled. Colchicine is necessary to both relieve symptoms and reduce the rate of recurrences and is continued for at least 3-6 months. Low- to moderate-dose glucocorticoids are reserved for patients with a first recurrence for which NSAIDs and colchicine failed and/or who have an autoimmune disorder, with a slow tapering. Interleukin-1 blockers-anakinra, rilonacept, and goflikicept-are used as a third-line option in patients who cannot come off glucocorticoids or as second-line therapy after NSAIDs and colchicine in patients with contraindications to glucocorticoids or in those with high-risk features (i.e., multiple episodes, markedly elevated inflammatory markers, or extensive abnormalities at pericardial imaging) in whom treatment with glucocorticoids is unlikely to succeed.
期刊介绍:
Drugs is a journal that aims to enhance pharmacotherapy by publishing review and original research articles on key aspects of clinical pharmacology and therapeutics. The journal includes:
Leading/current opinion articles providing an overview of contentious or emerging issues.
Definitive reviews of drugs and drug classes, and their place in disease management.
Therapy in Practice articles including recommendations for specific clinical situations.
High-quality, well designed, original clinical research.
Adis Drug Evaluations reviewing the properties and place in therapy of both newer and established drugs.
AdisInsight Reports summarising development at first global approval.
Moreover, the journal offers additional digital features such as animated abstracts, video abstracts, instructional videos, and podcasts to increase visibility and educational value. Plain language summaries accompany articles to assist readers with some knowledge of the field in understanding important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


