Martin C Lam, Vendela Grufman, Sonia Fertsch, Florian Recker, Nicole E Speck, Jian Farhadi
{"title":"乳房大小对BRCA突变携带者及遗传高危患者双侧乳房切除术后乳房重建的影响。","authors":"Martin C Lam, Vendela Grufman, Sonia Fertsch, Florian Recker, Nicole E Speck, Jian Farhadi","doi":"10.1007/s12282-025-01691-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Women with genetic susceptibility to breast cancer and indication for bilateral mastectomy are more likely to undergo implant-based breast reconstruction (IBR) than autologous breast reconstruction (ABR), while the impact of breast size in this context is insufficiently studied. Ultimately, comparative data on IBR and different types of ABR beyond abdominal-based flaps in genetic susceptible women remain scarce. This study aimed to evaluate factors associated with ABR and the effects of breast size for bilateral reconstruction in high-risk patients.</p><p><strong>Methods: </strong>A 2.5-year retrospective study was conducted at a single institution including all genetic high-risk patients who underwent bilateral mastectomy and breast reconstruction. Patients were stratified into two groups based on the weight of the mastectomy specimen. Small breast sizes were defined by mastectomy weights below 400 g, and medium-to-large breasts by specimen weights above 400 g. Binary logistic regression was performed to assess variables predictive of ABR, followed by an analysis of the breast size-dependent reconstructive algorithm and its complication rates.</p><p><strong>Results: </strong>We included 71 patients with BRCA1/2 (97.2%), CHEK2 (1.4%), and PALB2 (1.4%) mutations in the study. Among those, 68 IBRs and 74 ABRs were performed. Increasing age, immediate reconstruction, and medium-to-large breast size were predictive of ABR compared to IBR (p < 0.05). In the IBR-group, the majority of preoperative small breasts received subpectoral implant placements (81.0%, p = 0.003), while prepectoral implants (53.9%, p = 0.003) were preferred in medium-to-large breasts. In the ABR-group, the deep inferior epigastric artery (DIEP) flap was the choice in the vast majority of cases with larger breasts (86.4%, p < 0.001), whereas the transverse myocutaneous gracilis (TMG) flap (46.7%, p < 0.001) and superior gluteal artery perforator (SGAP) flap (20.0%, p = 0.002) were only considered in small-breasted patients. No elevated incidence of overall complications with increasing breast size was found. However, patients with larger breasts were more likely to undergo elective revisions after IBR (p < 0.001) as well as ABR (p = 0.013). With regard to two-stage tissue expander reconstructions, high-risk patients with larger breast size revealed increased explantations (p = 0.043) and expander-related revisions requiring additional surgery (p = 0.003). The latter was significantly reduced by reduction mammoplasty prior to expander placement (p = 0.036).</p><p><strong>Conclusions: </strong>The preoperative breast size of gene mutation carriers influences the postmastectomy reconstructive choice. TMG and SGAP flaps are suitable options for bilateral reconstruction of genetic susceptible patients with small breasts, while DIEP flaps are preferred in larger breast sizes. With increasing breast size an elevated risk for elective revisions after either IBR or ABR need to be considered. Women with medium-to-large breasts exhibit increased morbidity related to expansion and genetic high-risk patients may benefit from prior reduction mammoplasty.</p>","PeriodicalId":56083,"journal":{"name":"Breast Cancer","volume":" ","pages":"582-595"},"PeriodicalIF":2.9000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11993471/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of breast size on breast reconstruction in BRCA mutation carriers and genetic high-risk patients after bilateral mastectomy.\",\"authors\":\"Martin C Lam, Vendela Grufman, Sonia Fertsch, Florian Recker, Nicole E Speck, Jian Farhadi\",\"doi\":\"10.1007/s12282-025-01691-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Women with genetic susceptibility to breast cancer and indication for bilateral mastectomy are more likely to undergo implant-based breast reconstruction (IBR) than autologous breast reconstruction (ABR), while the impact of breast size in this context is insufficiently studied. Ultimately, comparative data on IBR and different types of ABR beyond abdominal-based flaps in genetic susceptible women remain scarce. This study aimed to evaluate factors associated with ABR and the effects of breast size for bilateral reconstruction in high-risk patients.</p><p><strong>Methods: </strong>A 2.5-year retrospective study was conducted at a single institution including all genetic high-risk patients who underwent bilateral mastectomy and breast reconstruction. Patients were stratified into two groups based on the weight of the mastectomy specimen. Small breast sizes were defined by mastectomy weights below 400 g, and medium-to-large breasts by specimen weights above 400 g. Binary logistic regression was performed to assess variables predictive of ABR, followed by an analysis of the breast size-dependent reconstructive algorithm and its complication rates.</p><p><strong>Results: </strong>We included 71 patients with BRCA1/2 (97.2%), CHEK2 (1.4%), and PALB2 (1.4%) mutations in the study. Among those, 68 IBRs and 74 ABRs were performed. Increasing age, immediate reconstruction, and medium-to-large breast size were predictive of ABR compared to IBR (p < 0.05). In the IBR-group, the majority of preoperative small breasts received subpectoral implant placements (81.0%, p = 0.003), while prepectoral implants (53.9%, p = 0.003) were preferred in medium-to-large breasts. In the ABR-group, the deep inferior epigastric artery (DIEP) flap was the choice in the vast majority of cases with larger breasts (86.4%, p < 0.001), whereas the transverse myocutaneous gracilis (TMG) flap (46.7%, p < 0.001) and superior gluteal artery perforator (SGAP) flap (20.0%, p = 0.002) were only considered in small-breasted patients. No elevated incidence of overall complications with increasing breast size was found. However, patients with larger breasts were more likely to undergo elective revisions after IBR (p < 0.001) as well as ABR (p = 0.013). With regard to two-stage tissue expander reconstructions, high-risk patients with larger breast size revealed increased explantations (p = 0.043) and expander-related revisions requiring additional surgery (p = 0.003). The latter was significantly reduced by reduction mammoplasty prior to expander placement (p = 0.036).</p><p><strong>Conclusions: </strong>The preoperative breast size of gene mutation carriers influences the postmastectomy reconstructive choice. TMG and SGAP flaps are suitable options for bilateral reconstruction of genetic susceptible patients with small breasts, while DIEP flaps are preferred in larger breast sizes. With increasing breast size an elevated risk for elective revisions after either IBR or ABR need to be considered. Women with medium-to-large breasts exhibit increased morbidity related to expansion and genetic high-risk patients may benefit from prior reduction mammoplasty.</p>\",\"PeriodicalId\":56083,\"journal\":{\"name\":\"Breast Cancer\",\"volume\":\" \",\"pages\":\"582-595\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11993471/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Breast Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12282-025-01691-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12282-025-01691-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Effects of breast size on breast reconstruction in BRCA mutation carriers and genetic high-risk patients after bilateral mastectomy.
Background: Women with genetic susceptibility to breast cancer and indication for bilateral mastectomy are more likely to undergo implant-based breast reconstruction (IBR) than autologous breast reconstruction (ABR), while the impact of breast size in this context is insufficiently studied. Ultimately, comparative data on IBR and different types of ABR beyond abdominal-based flaps in genetic susceptible women remain scarce. This study aimed to evaluate factors associated with ABR and the effects of breast size for bilateral reconstruction in high-risk patients.
Methods: A 2.5-year retrospective study was conducted at a single institution including all genetic high-risk patients who underwent bilateral mastectomy and breast reconstruction. Patients were stratified into two groups based on the weight of the mastectomy specimen. Small breast sizes were defined by mastectomy weights below 400 g, and medium-to-large breasts by specimen weights above 400 g. Binary logistic regression was performed to assess variables predictive of ABR, followed by an analysis of the breast size-dependent reconstructive algorithm and its complication rates.
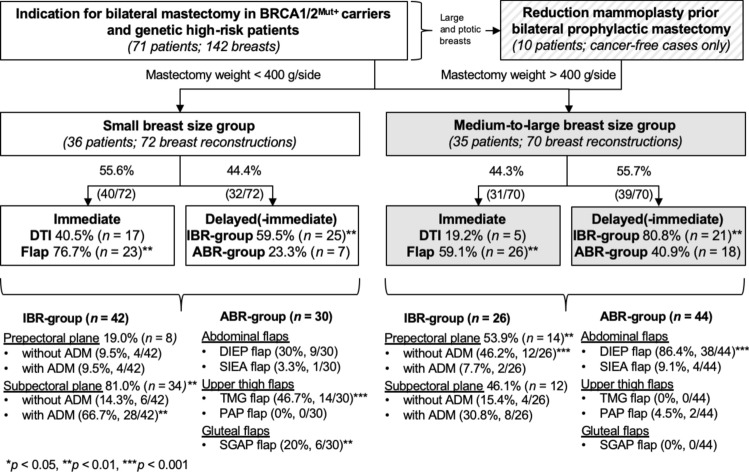
Results: We included 71 patients with BRCA1/2 (97.2%), CHEK2 (1.4%), and PALB2 (1.4%) mutations in the study. Among those, 68 IBRs and 74 ABRs were performed. Increasing age, immediate reconstruction, and medium-to-large breast size were predictive of ABR compared to IBR (p < 0.05). In the IBR-group, the majority of preoperative small breasts received subpectoral implant placements (81.0%, p = 0.003), while prepectoral implants (53.9%, p = 0.003) were preferred in medium-to-large breasts. In the ABR-group, the deep inferior epigastric artery (DIEP) flap was the choice in the vast majority of cases with larger breasts (86.4%, p < 0.001), whereas the transverse myocutaneous gracilis (TMG) flap (46.7%, p < 0.001) and superior gluteal artery perforator (SGAP) flap (20.0%, p = 0.002) were only considered in small-breasted patients. No elevated incidence of overall complications with increasing breast size was found. However, patients with larger breasts were more likely to undergo elective revisions after IBR (p < 0.001) as well as ABR (p = 0.013). With regard to two-stage tissue expander reconstructions, high-risk patients with larger breast size revealed increased explantations (p = 0.043) and expander-related revisions requiring additional surgery (p = 0.003). The latter was significantly reduced by reduction mammoplasty prior to expander placement (p = 0.036).
Conclusions: The preoperative breast size of gene mutation carriers influences the postmastectomy reconstructive choice. TMG and SGAP flaps are suitable options for bilateral reconstruction of genetic susceptible patients with small breasts, while DIEP flaps are preferred in larger breast sizes. With increasing breast size an elevated risk for elective revisions after either IBR or ABR need to be considered. Women with medium-to-large breasts exhibit increased morbidity related to expansion and genetic high-risk patients may benefit from prior reduction mammoplasty.
期刊介绍:
Breast Cancer, the official journal of the Japanese Breast Cancer Society, publishes articles that contribute to progress in the field, in basic or translational research and also in clinical research, seeking to develop a new focus and new perspectives for all who are concerned with breast cancer. The journal welcomes all original articles describing clinical and epidemiological studies and laboratory investigations regarding breast cancer and related diseases. The journal will consider five types of articles: editorials, review articles, original articles, case reports, and rapid communications. Although editorials and review articles will principally be solicited by the editors, they can also be submitted for peer review, as in the case of original articles. The journal provides the best of up-to-date information on breast cancer, presenting readers with high-impact, original work focusing on pivotal issues.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


