{"title":"与后肠复制异常相关的泄殖腔外翻:后肠保存挑战的一例报告。","authors":"Suliaman Alaqeel, Jamila Almaary, Fatmah Alrabodh, Fayez AlModhen","doi":"10.1055/a-2544-3341","DOIUrl":null,"url":null,"abstract":"<p><p>Cloacal exstrophy (CE) is a rare condition, and the preservation of a short hindgut is crucial for growth, fluid-electrolyte balance, and bowel management. Herein, we present the case of an infant with concurrent anomalies and the challenges faced during the preservation of both hindguts. A preterm male infant, born at 34 weeks weighing 2 kg, was diagnosed with CE. The first stage of CE repair was performed at 3 months of age, involving the separation and tubularization of the cecal plate and the joining of the two hemi-bladders. During the procedure, hindgut duplication was noted. Each hindgut had a short mesentery with far-separated, tiny blind ends (7 and 10 cm in length), each directed toward opposite sides of the pelvis and measuring 8 Fr in caliber. Due to the risk of compromising the blood supply during rotation and mobilization of one hindgut, the decision was made to exteriorize each hindgut as end stomas. Both stomas began functioning as expected. However, a colo-cutaneous fistula (connecting the cecum to the midline surgical wound) developed and was managed conservatively for 8 weeks. During this period, despite the functioning left stoma, the right stoma was stenosed, and the fistula persisted. The infant underwent a second laparotomy for fistula repair and reconstruction of both hindguts. This was successfully managed by creating a single-lumen end stoma, preserving the entire length of the hindguts with a wider caliber. In conclusion, complex cases of CE are uncommon, and unexpected operative findings should always be anticipated. Reconstructing both hindguts into a single lumen during the initial procedure can be challenging but is achievable with time and careful effort. Preservation of both hindgut ends should be prioritized. However, long-term outcomes remain uncertain due to the rarity of this presentation.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"13 1","pages":"e1-e3"},"PeriodicalIF":0.7000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919476/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cloacal Exstrophy Associated with a Hindgut Duplication Anomaly: A Case Report of Challenges in Hindgut Preservation.\",\"authors\":\"Suliaman Alaqeel, Jamila Almaary, Fatmah Alrabodh, Fayez AlModhen\",\"doi\":\"10.1055/a-2544-3341\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cloacal exstrophy (CE) is a rare condition, and the preservation of a short hindgut is crucial for growth, fluid-electrolyte balance, and bowel management. Herein, we present the case of an infant with concurrent anomalies and the challenges faced during the preservation of both hindguts. A preterm male infant, born at 34 weeks weighing 2 kg, was diagnosed with CE. The first stage of CE repair was performed at 3 months of age, involving the separation and tubularization of the cecal plate and the joining of the two hemi-bladders. During the procedure, hindgut duplication was noted. Each hindgut had a short mesentery with far-separated, tiny blind ends (7 and 10 cm in length), each directed toward opposite sides of the pelvis and measuring 8 Fr in caliber. Due to the risk of compromising the blood supply during rotation and mobilization of one hindgut, the decision was made to exteriorize each hindgut as end stomas. Both stomas began functioning as expected. However, a colo-cutaneous fistula (connecting the cecum to the midline surgical wound) developed and was managed conservatively for 8 weeks. During this period, despite the functioning left stoma, the right stoma was stenosed, and the fistula persisted. The infant underwent a second laparotomy for fistula repair and reconstruction of both hindguts. This was successfully managed by creating a single-lumen end stoma, preserving the entire length of the hindguts with a wider caliber. In conclusion, complex cases of CE are uncommon, and unexpected operative findings should always be anticipated. Reconstructing both hindguts into a single lumen during the initial procedure can be challenging but is achievable with time and careful effort. Preservation of both hindgut ends should be prioritized. However, long-term outcomes remain uncertain due to the rarity of this presentation.</p>\",\"PeriodicalId\":43204,\"journal\":{\"name\":\"European Journal of Pediatric Surgery Reports\",\"volume\":\"13 1\",\"pages\":\"e1-e3\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-03-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11919476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pediatric Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2544-3341\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2544-3341","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Cloacal Exstrophy Associated with a Hindgut Duplication Anomaly: A Case Report of Challenges in Hindgut Preservation.
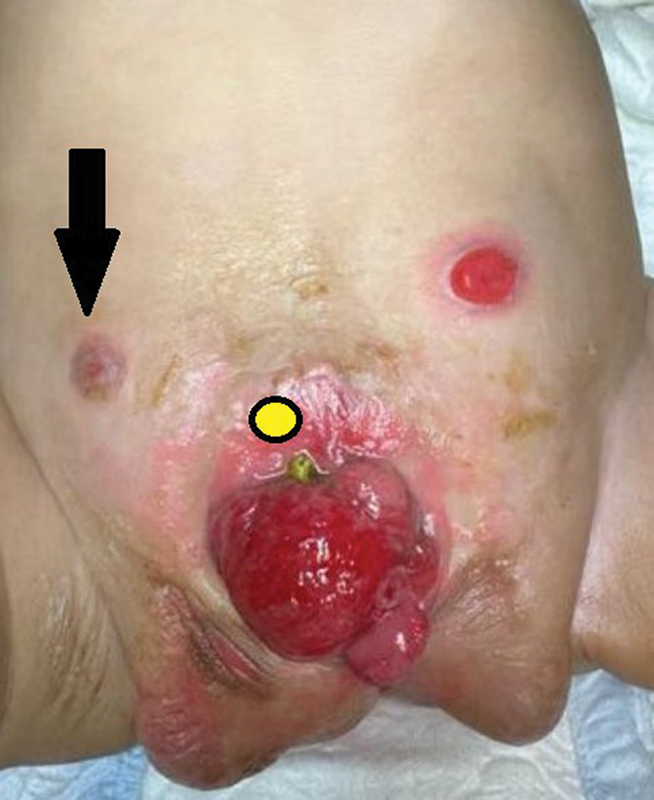
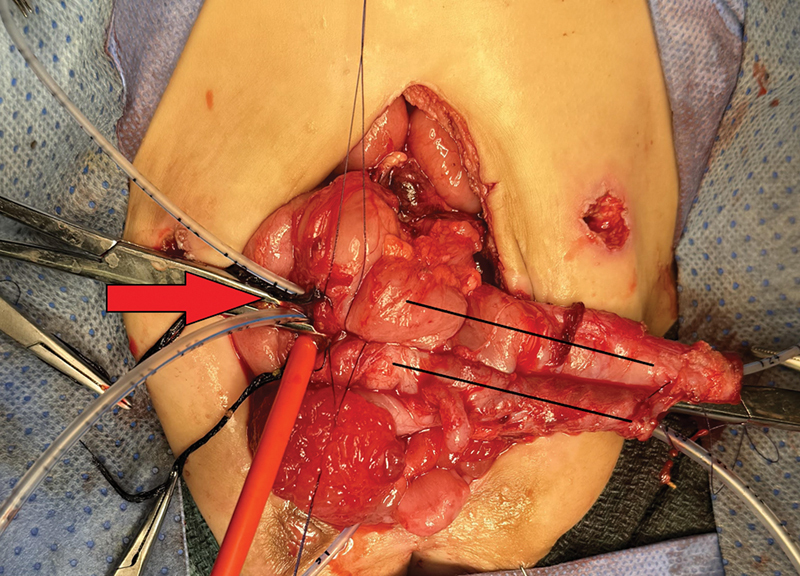
Cloacal exstrophy (CE) is a rare condition, and the preservation of a short hindgut is crucial for growth, fluid-electrolyte balance, and bowel management. Herein, we present the case of an infant with concurrent anomalies and the challenges faced during the preservation of both hindguts. A preterm male infant, born at 34 weeks weighing 2 kg, was diagnosed with CE. The first stage of CE repair was performed at 3 months of age, involving the separation and tubularization of the cecal plate and the joining of the two hemi-bladders. During the procedure, hindgut duplication was noted. Each hindgut had a short mesentery with far-separated, tiny blind ends (7 and 10 cm in length), each directed toward opposite sides of the pelvis and measuring 8 Fr in caliber. Due to the risk of compromising the blood supply during rotation and mobilization of one hindgut, the decision was made to exteriorize each hindgut as end stomas. Both stomas began functioning as expected. However, a colo-cutaneous fistula (connecting the cecum to the midline surgical wound) developed and was managed conservatively for 8 weeks. During this period, despite the functioning left stoma, the right stoma was stenosed, and the fistula persisted. The infant underwent a second laparotomy for fistula repair and reconstruction of both hindguts. This was successfully managed by creating a single-lumen end stoma, preserving the entire length of the hindguts with a wider caliber. In conclusion, complex cases of CE are uncommon, and unexpected operative findings should always be anticipated. Reconstructing both hindguts into a single lumen during the initial procedure can be challenging but is achievable with time and careful effort. Preservation of both hindgut ends should be prioritized. However, long-term outcomes remain uncertain due to the rarity of this presentation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


