Gaohua Wu, Xiufen Chen, Rongkui Luo, Ye Xin Koh, Tony Kiat Hon Lim, Valerie Chew, Jian Zhou, Jia Fan, Qiang Gao, Kai Zhu, Ruoyu Shi
{"title":"残余肿瘤的组织病理学分级预测新辅助治疗肝内胆管癌患者的生存:主要病理反应及其临床意义。","authors":"Gaohua Wu, Xiufen Chen, Rongkui Luo, Ye Xin Koh, Tony Kiat Hon Lim, Valerie Chew, Jian Zhou, Jia Fan, Qiang Gao, Kai Zhu, Ruoyu Shi","doi":"10.1097/PAS.0000000000002359","DOIUrl":null,"url":null,"abstract":"<p><p>Neoadjuvant therapy (NAT) is increasingly used to treat patients with initially unresectable intrahepatic cholangiocarcinoma (iCCA). A histopathologic grading system for residual tumors that can predict patient survival is lacking in the literature. This retrospective study enrolled 151 iCCA patients who received NAT. The percentage of residual viable tumor (%RVT) extent was calculated by RVT surface area/total tumor bed area ×100 and scored in 5% increments. Kaplan-Meier and Cox regression analyses were used to investigate its correlations with recurrence-free survival (RFS) and overall survival (OS). Tumor regression grading by the College of American Pathologists (CAP) and MD Anderson (MDA) methodologies were also validated. A 10% RVT-based tumor regression score (TRS) showed a significant correlation with both OS and RFS. TRS and major pathologic response (mPR) were therefore defined as follows: TRS 1/mPR, tumor with 0 to 10% RVT; TRS 2, more than 10% RVT. Patients graded as TRS 1/mPR had superior OS ( P =0.006) and RFS ( P <0.001) compared with those with TRS 2 in univariate analysis. In a multivariate analysis including ypTNM stages, lymphovascular invasion, and perineural invasion, TRS 1/mPR was also found to be an independent prognostic factor for both OS (hazard ratio [HR]: 0.226; 95% CI: 0.053-0.966, P =0.045) and RFS (HR: 0.474; 95% CI: 0.231-0.974, P =0.042). As for the CAP and MDA grading methodologies, they were found to correlate with RFS (CAP: P =0.002; MDA: P =0.001), but not with OS (CAP: P =0.181; MDA: P =0.09). Our study revealed that a TRS of ≤10% RVT significantly correlates with longer OS and RFS and can be suggested as an mPR in iCCA. This indicator is easily applicable, prognostically relevant, and could be further validated in future prospective clinical trials.</p>","PeriodicalId":7772,"journal":{"name":"American Journal of Surgical Pathology","volume":" ","pages":"578-587"},"PeriodicalIF":4.2000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068548/pdf/","citationCount":"0","resultStr":"{\"title\":\"Histopathologic Grading of Residual Tumor Predicts Survival of Intrahepatic Cholangiocarcinoma Patients Treated With Neoadjuvant Therapy: Major Pathologic Response and Its Clinical Significance.\",\"authors\":\"Gaohua Wu, Xiufen Chen, Rongkui Luo, Ye Xin Koh, Tony Kiat Hon Lim, Valerie Chew, Jian Zhou, Jia Fan, Qiang Gao, Kai Zhu, Ruoyu Shi\",\"doi\":\"10.1097/PAS.0000000000002359\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Neoadjuvant therapy (NAT) is increasingly used to treat patients with initially unresectable intrahepatic cholangiocarcinoma (iCCA). A histopathologic grading system for residual tumors that can predict patient survival is lacking in the literature. This retrospective study enrolled 151 iCCA patients who received NAT. The percentage of residual viable tumor (%RVT) extent was calculated by RVT surface area/total tumor bed area ×100 and scored in 5% increments. Kaplan-Meier and Cox regression analyses were used to investigate its correlations with recurrence-free survival (RFS) and overall survival (OS). Tumor regression grading by the College of American Pathologists (CAP) and MD Anderson (MDA) methodologies were also validated. A 10% RVT-based tumor regression score (TRS) showed a significant correlation with both OS and RFS. TRS and major pathologic response (mPR) were therefore defined as follows: TRS 1/mPR, tumor with 0 to 10% RVT; TRS 2, more than 10% RVT. Patients graded as TRS 1/mPR had superior OS ( P =0.006) and RFS ( P <0.001) compared with those with TRS 2 in univariate analysis. In a multivariate analysis including ypTNM stages, lymphovascular invasion, and perineural invasion, TRS 1/mPR was also found to be an independent prognostic factor for both OS (hazard ratio [HR]: 0.226; 95% CI: 0.053-0.966, P =0.045) and RFS (HR: 0.474; 95% CI: 0.231-0.974, P =0.042). As for the CAP and MDA grading methodologies, they were found to correlate with RFS (CAP: P =0.002; MDA: P =0.001), but not with OS (CAP: P =0.181; MDA: P =0.09). Our study revealed that a TRS of ≤10% RVT significantly correlates with longer OS and RFS and can be suggested as an mPR in iCCA. This indicator is easily applicable, prognostically relevant, and could be further validated in future prospective clinical trials.</p>\",\"PeriodicalId\":7772,\"journal\":{\"name\":\"American Journal of Surgical Pathology\",\"volume\":\" \",\"pages\":\"578-587\"},\"PeriodicalIF\":4.2000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068548/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Surgical Pathology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/PAS.0000000000002359\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Surgical Pathology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/PAS.0000000000002359","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
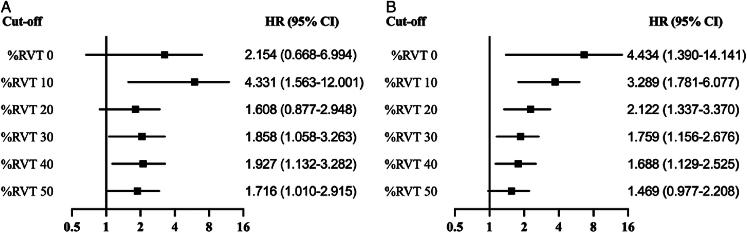
新辅助治疗(NAT)越来越多地用于治疗最初不可切除的肝内胆管癌(iCCA)患者。文献中缺乏残留肿瘤的组织病理学分级系统来预测患者的生存。本回顾性研究纳入151例接受NAT治疗的iCCA患者。剩余活肿瘤百分比(%RVT)范围由RVT表面积/总肿瘤床面积×100计算,以5%的增量评分。采用Kaplan-Meier和Cox回归分析探讨其与无复发生存期(RFS)和总生存期(OS)的相关性。美国病理学家学会(CAP)和MD Anderson (MDA)方法的肿瘤消退分级也得到了验证。10%基于rvt的肿瘤回归评分(TRS)与OS和RFS均有显著相关性。因此,TRS和主要病理反应(mPR)的定义如下:TRS 1/mPR为RVT为0 ~ 10%的肿瘤;TRS 2, RVT大于10%。TRS分级为1/mPR的患者有较好的OS (P=0.006)和RFS (P=0.006)
Histopathologic Grading of Residual Tumor Predicts Survival of Intrahepatic Cholangiocarcinoma Patients Treated With Neoadjuvant Therapy: Major Pathologic Response and Its Clinical Significance.
Neoadjuvant therapy (NAT) is increasingly used to treat patients with initially unresectable intrahepatic cholangiocarcinoma (iCCA). A histopathologic grading system for residual tumors that can predict patient survival is lacking in the literature. This retrospective study enrolled 151 iCCA patients who received NAT. The percentage of residual viable tumor (%RVT) extent was calculated by RVT surface area/total tumor bed area ×100 and scored in 5% increments. Kaplan-Meier and Cox regression analyses were used to investigate its correlations with recurrence-free survival (RFS) and overall survival (OS). Tumor regression grading by the College of American Pathologists (CAP) and MD Anderson (MDA) methodologies were also validated. A 10% RVT-based tumor regression score (TRS) showed a significant correlation with both OS and RFS. TRS and major pathologic response (mPR) were therefore defined as follows: TRS 1/mPR, tumor with 0 to 10% RVT; TRS 2, more than 10% RVT. Patients graded as TRS 1/mPR had superior OS ( P =0.006) and RFS ( P <0.001) compared with those with TRS 2 in univariate analysis. In a multivariate analysis including ypTNM stages, lymphovascular invasion, and perineural invasion, TRS 1/mPR was also found to be an independent prognostic factor for both OS (hazard ratio [HR]: 0.226; 95% CI: 0.053-0.966, P =0.045) and RFS (HR: 0.474; 95% CI: 0.231-0.974, P =0.042). As for the CAP and MDA grading methodologies, they were found to correlate with RFS (CAP: P =0.002; MDA: P =0.001), but not with OS (CAP: P =0.181; MDA: P =0.09). Our study revealed that a TRS of ≤10% RVT significantly correlates with longer OS and RFS and can be suggested as an mPR in iCCA. This indicator is easily applicable, prognostically relevant, and could be further validated in future prospective clinical trials.
期刊介绍:
The American Journal of Surgical Pathology has achieved worldwide recognition for its outstanding coverage of the state of the art in human surgical pathology. In each monthly issue, experts present original articles, review articles, detailed case reports, and special features, enhanced by superb illustrations. Coverage encompasses technical methods, diagnostic aids, and frozen-section diagnosis, in addition to detailed pathologic studies of a wide range of disease entities.
Official Journal of The Arthur Purdy Stout Society of Surgical Pathologists and The Gastrointestinal Pathology Society.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


