Ahmed Ezzat, Dhurka Shanthakumar, Naomi Laskar, Ramsey I Cutress, Dimitri Hadjiminas, Michael Boland, Meera Joshi, Ronak Patel, Yasmin Grant, Ravi Naik, Nur Amalina Che Bakri, Saur Hajev, Hussein Elghazaly, Josephine Holt, Alfie Roddan, Susan Cleator, Ara Darzi, Hutan Ashrafian, Daniel R Leff
{"title":"纯导管原位癌保乳手术和全乳放疗后切除边缘宽度对局部复发的影响:系统回顾和荟萃分析。","authors":"Ahmed Ezzat, Dhurka Shanthakumar, Naomi Laskar, Ramsey I Cutress, Dimitri Hadjiminas, Michael Boland, Meera Joshi, Ronak Patel, Yasmin Grant, Ravi Naik, Nur Amalina Che Bakri, Saur Hajev, Hussein Elghazaly, Josephine Holt, Alfie Roddan, Susan Cleator, Ara Darzi, Hutan Ashrafian, Daniel R Leff","doi":"10.1136/bmjonc-2024-000633","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of this study was to determine the impact of margin width and boost radiotherapy on the local recurrence risk of pure ductal carcinoma in situ (DCIS).</p><p><strong>Methods and analysis: </strong>This is a prospectively registered systematic review and meta-analysis reporting relative risk (RR), OR and HR margin width outcomes. Eligible studies included prospective and retrospective case series with defining margin widths and 48 months of minimum follow-up. All patients (100%) received adjuvant whole breast radiotherapy (WBRT).</p><p><strong>Results: </strong>A total of 40 265 patients with pure DCIS in 31 studies were included. ORs and RR were calculated from 15 studies in 12 519 patients, and HRs were calculated from 12 studies in 12 946 patients. Local recurrence was significantly greater with narrower 'close' margins; 0.1-1 mm versus >1 mm in RR (2.88, 95% CI 1.86 to 3.90; p<0.05), OR (4.82, 95% CI 2.45 to 9.48; p<0.05) and HR analysis (1.34, 95% CI 1.01 to 1.67; p<0.05). Compared with margins >2 mm, significantly greater local recurrence was observed in margins 0.1-2 mm in RR (1.72, 95% CI 1.09 to 2.35; p<0.05) and OR (4.43, 95% CI 3.02 to 6.50; p<0.05). Comparing 0.1-1 mm versus >1 mm and 0.1-2 mm versus >2 mm, differences in local recurrence were not statistically significant, once adjusted for boost radiotherapy.</p><p><strong>Conclusions: </strong>In pure DCIS with WBRT, the local recurrence risk reduces as margin width increases up to 2 mm. The strength of the recommendation for a minimum clear margin of 2 mm is limited by a lack of data comparing 1.1-2 mm with >2 mm. The association between recurrence and close margins is not significant following boost radiotherapy, suggesting a possible alternative to re-excision in patients with close margins <2 mm.</p><p><strong>Systematic review registration: </strong>CRD42022308524.</p>","PeriodicalId":72436,"journal":{"name":"BMJ oncology","volume":"4 1","pages":"e000633"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11911704/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of resection margin width on local recurrence following breast-conserving surgery and whole breast radiotherapy for pure ductal carcinoma in situ: a systematic review and meta-analysis.\",\"authors\":\"Ahmed Ezzat, Dhurka Shanthakumar, Naomi Laskar, Ramsey I Cutress, Dimitri Hadjiminas, Michael Boland, Meera Joshi, Ronak Patel, Yasmin Grant, Ravi Naik, Nur Amalina Che Bakri, Saur Hajev, Hussein Elghazaly, Josephine Holt, Alfie Roddan, Susan Cleator, Ara Darzi, Hutan Ashrafian, Daniel R Leff\",\"doi\":\"10.1136/bmjonc-2024-000633\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim of this study was to determine the impact of margin width and boost radiotherapy on the local recurrence risk of pure ductal carcinoma in situ (DCIS).</p><p><strong>Methods and analysis: </strong>This is a prospectively registered systematic review and meta-analysis reporting relative risk (RR), OR and HR margin width outcomes. Eligible studies included prospective and retrospective case series with defining margin widths and 48 months of minimum follow-up. All patients (100%) received adjuvant whole breast radiotherapy (WBRT).</p><p><strong>Results: </strong>A total of 40 265 patients with pure DCIS in 31 studies were included. ORs and RR were calculated from 15 studies in 12 519 patients, and HRs were calculated from 12 studies in 12 946 patients. Local recurrence was significantly greater with narrower 'close' margins; 0.1-1 mm versus >1 mm in RR (2.88, 95% CI 1.86 to 3.90; p<0.05), OR (4.82, 95% CI 2.45 to 9.48; p<0.05) and HR analysis (1.34, 95% CI 1.01 to 1.67; p<0.05). Compared with margins >2 mm, significantly greater local recurrence was observed in margins 0.1-2 mm in RR (1.72, 95% CI 1.09 to 2.35; p<0.05) and OR (4.43, 95% CI 3.02 to 6.50; p<0.05). Comparing 0.1-1 mm versus >1 mm and 0.1-2 mm versus >2 mm, differences in local recurrence were not statistically significant, once adjusted for boost radiotherapy.</p><p><strong>Conclusions: </strong>In pure DCIS with WBRT, the local recurrence risk reduces as margin width increases up to 2 mm. The strength of the recommendation for a minimum clear margin of 2 mm is limited by a lack of data comparing 1.1-2 mm with >2 mm. The association between recurrence and close margins is not significant following boost radiotherapy, suggesting a possible alternative to re-excision in patients with close margins <2 mm.</p><p><strong>Systematic review registration: </strong>CRD42022308524.</p>\",\"PeriodicalId\":72436,\"journal\":{\"name\":\"BMJ oncology\",\"volume\":\"4 1\",\"pages\":\"e000633\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11911704/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjonc-2024-000633\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjonc-2024-000633","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
研究目的本研究旨在确定边缘宽度和增强放疗对纯导管原位癌(DCIS)局部复发风险的影响:这是一项前瞻性注册的系统综述和荟萃分析,报告了边缘宽度结果的相对风险(RR)、OR和HR。符合条件的研究包括确定边缘宽度的前瞻性和回顾性病例系列,随访时间至少48个月。所有患者(100%)均接受了辅助性全乳腺放疗(WBRT):结果:共纳入了 31 项研究中的 40 265 例纯 DCIS 患者。15 项研究计算了 12 519 例患者的 OR 和 RR,12 项研究计算了 12 946 例患者的 HR。局部复发率在边缘较窄的情况下明显增加;0.1-1毫米与>1毫米的RR(2.88,95% CI 1.86至3.90;p2毫米),在边缘0.1-2毫米的RR(1.72,95% CI 1.09至2.35;p1毫米)和0.1-2毫米与>2毫米的RR(1.72,95% CI 1.09至2.35;p1毫米)中观察到局部复发率明显增加,在调整了增强放疗后,局部复发率的差异无统计学意义:结论:对纯DCIS进行WBRT治疗,局部复发风险随着边缘宽度的增加而降低,最大可达2毫米。由于缺乏1.1-2毫米与>2毫米之间的比较数据,建议最小清晰边缘为2毫米的力度受到了限制。增强放疗后,复发与切缘过近之间的关系并不显著,这表明切缘过近的患者可以选择再次切除:CRD42022308524。
Impact of resection margin width on local recurrence following breast-conserving surgery and whole breast radiotherapy for pure ductal carcinoma in situ: a systematic review and meta-analysis.
Objective: The aim of this study was to determine the impact of margin width and boost radiotherapy on the local recurrence risk of pure ductal carcinoma in situ (DCIS).
Methods and analysis: This is a prospectively registered systematic review and meta-analysis reporting relative risk (RR), OR and HR margin width outcomes. Eligible studies included prospective and retrospective case series with defining margin widths and 48 months of minimum follow-up. All patients (100%) received adjuvant whole breast radiotherapy (WBRT).
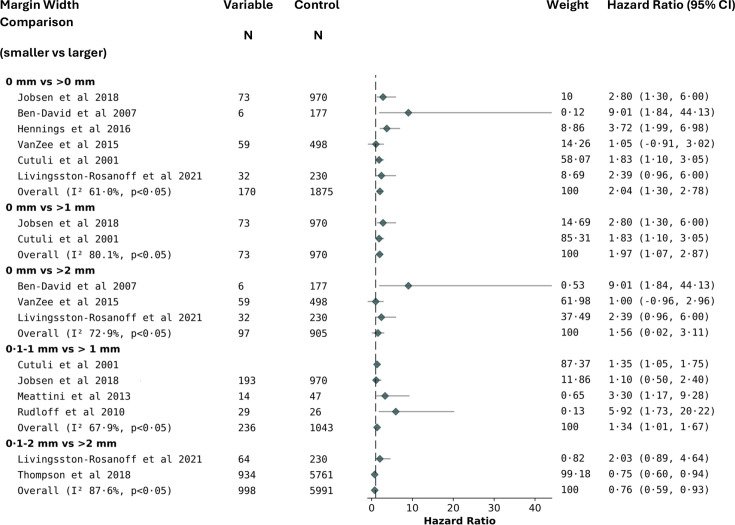
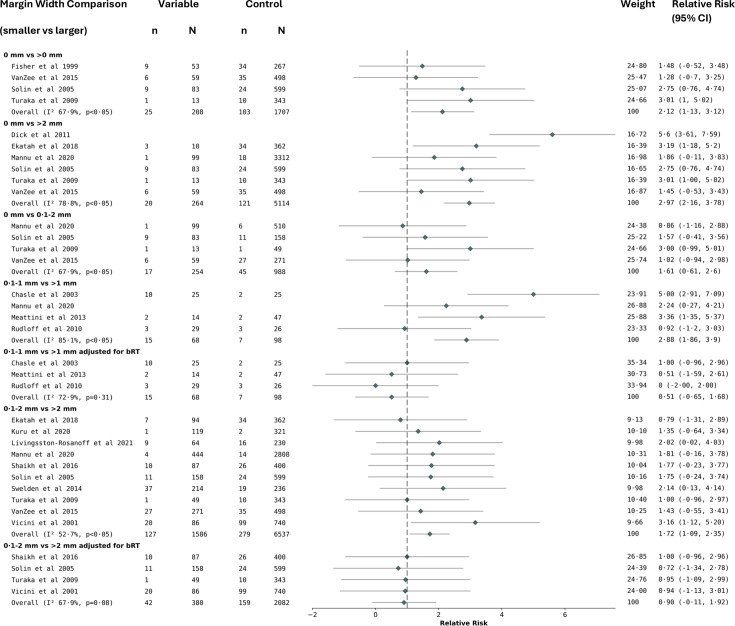
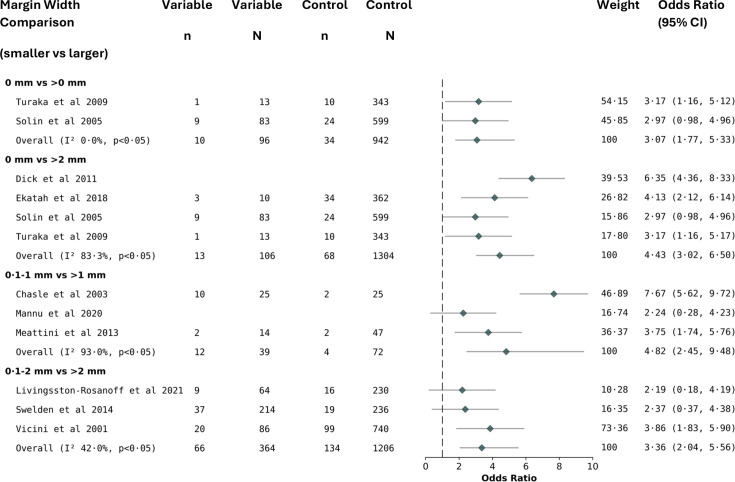
Results: A total of 40 265 patients with pure DCIS in 31 studies were included. ORs and RR were calculated from 15 studies in 12 519 patients, and HRs were calculated from 12 studies in 12 946 patients. Local recurrence was significantly greater with narrower 'close' margins; 0.1-1 mm versus >1 mm in RR (2.88, 95% CI 1.86 to 3.90; p<0.05), OR (4.82, 95% CI 2.45 to 9.48; p<0.05) and HR analysis (1.34, 95% CI 1.01 to 1.67; p<0.05). Compared with margins >2 mm, significantly greater local recurrence was observed in margins 0.1-2 mm in RR (1.72, 95% CI 1.09 to 2.35; p<0.05) and OR (4.43, 95% CI 3.02 to 6.50; p<0.05). Comparing 0.1-1 mm versus >1 mm and 0.1-2 mm versus >2 mm, differences in local recurrence were not statistically significant, once adjusted for boost radiotherapy.
Conclusions: In pure DCIS with WBRT, the local recurrence risk reduces as margin width increases up to 2 mm. The strength of the recommendation for a minimum clear margin of 2 mm is limited by a lack of data comparing 1.1-2 mm with >2 mm. The association between recurrence and close margins is not significant following boost radiotherapy, suggesting a possible alternative to re-excision in patients with close margins <2 mm.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


