Xiaojing Wang, Yuli Wang, Yiping Zhao, Yinan Li, Xiangjiang Guo, Lan Zhang, Jiaquan Chen, Qihong Ni
{"title":"臂丛阻滞与局部麻醉对功能障碍动静脉瘘的经皮腔内血管成形术:倾向评分加权研究的12个月结果。","authors":"Xiaojing Wang, Yuli Wang, Yiping Zhao, Yinan Li, Xiangjiang Guo, Lan Zhang, Jiaquan Chen, Qihong Ni","doi":"10.1080/0886022X.2025.2477834","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study aimed to compare ultrasound-guided brachial plexus block (BPB) with local anesthesia (LA) on efficacy, safety and 12-month patency rate for percutaneous transluminal angioplasty (PTA) treatment of dysfunctional arteriovenous fistula (AVF).</p><p><strong>Methods: </strong>Consecutive patients with dysfunctional AVF who underwent PTA from January 2021 to December 2022 were included. Overlap weighting was performed to adjust for significant differences between the two groups. The primary efficacy outcomes included visual analogue scale (VAS) score and 12-month target-lesion primary patency rate. The secondary efficacy outcomes included target-lesion primary-assisted patency rate, secondary patency rate, access-circuit thrombosis rate, access-circuit reintervention rate, and number of reinterventions within 12 months. Univariate analysis and multivariate analysis by log-binomial regression were used to identify the independent factors associated with intraoperative pain.</p><p><strong>Results: </strong>218 patients were included in the study: 82 patients underwent PTA under BPB and 136 patients underwent PTA under LA. After overlap weighting, the baseline, lesion characteristics and intraoperative details had no significant difference between the two groups. Patients under BPB had significantly lower VAS scores than those under LA (2.4 ± 1.4 vs 5.1 ± 1.9, <i>p</i> < 0.001). The 12-month target-lesion primary patency rate was significantly higher in the BPB group than that in the LA group (58.3% vs 40.0%, <i>p</i> = 0.037). The 12-month target-lesion primary-assisted patency rate and access-circuit secondary patency rate were significantly higher in the BPB group than those in the LA group (<i>p</i> = 0.023 and <i>p</i> = 0.028). The access-circuit thrombosis rate was significantly lower in the BPB group (10.0%) than that in the LA group (28.3%) (<i>p</i> = 0.011). BPB was the only independent factor associated with mild pain (<i>p</i> < 0.001, OR: 0.037, 95%CI: 0.011-0.119).</p><p><strong>Conclusions: </strong>BPB could decrease the intraoperative pain and improve the 12-month primary patency rates compared with LA for patients underwent PTA treatment of dysfunctional AVF.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"47 1","pages":"2477834"},"PeriodicalIF":3.0000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915726/pdf/","citationCount":"0","resultStr":"{\"title\":\"Brachial plexus block versus local anesthesia for percutaneous transluminal angioplasty of dysfunctional arteriovenous fistula: 12-month results of a propensity score weighted study.\",\"authors\":\"Xiaojing Wang, Yuli Wang, Yiping Zhao, Yinan Li, Xiangjiang Guo, Lan Zhang, Jiaquan Chen, Qihong Ni\",\"doi\":\"10.1080/0886022X.2025.2477834\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The study aimed to compare ultrasound-guided brachial plexus block (BPB) with local anesthesia (LA) on efficacy, safety and 12-month patency rate for percutaneous transluminal angioplasty (PTA) treatment of dysfunctional arteriovenous fistula (AVF).</p><p><strong>Methods: </strong>Consecutive patients with dysfunctional AVF who underwent PTA from January 2021 to December 2022 were included. Overlap weighting was performed to adjust for significant differences between the two groups. The primary efficacy outcomes included visual analogue scale (VAS) score and 12-month target-lesion primary patency rate. The secondary efficacy outcomes included target-lesion primary-assisted patency rate, secondary patency rate, access-circuit thrombosis rate, access-circuit reintervention rate, and number of reinterventions within 12 months. Univariate analysis and multivariate analysis by log-binomial regression were used to identify the independent factors associated with intraoperative pain.</p><p><strong>Results: </strong>218 patients were included in the study: 82 patients underwent PTA under BPB and 136 patients underwent PTA under LA. After overlap weighting, the baseline, lesion characteristics and intraoperative details had no significant difference between the two groups. Patients under BPB had significantly lower VAS scores than those under LA (2.4 ± 1.4 vs 5.1 ± 1.9, <i>p</i> < 0.001). The 12-month target-lesion primary patency rate was significantly higher in the BPB group than that in the LA group (58.3% vs 40.0%, <i>p</i> = 0.037). The 12-month target-lesion primary-assisted patency rate and access-circuit secondary patency rate were significantly higher in the BPB group than those in the LA group (<i>p</i> = 0.023 and <i>p</i> = 0.028). The access-circuit thrombosis rate was significantly lower in the BPB group (10.0%) than that in the LA group (28.3%) (<i>p</i> = 0.011). BPB was the only independent factor associated with mild pain (<i>p</i> < 0.001, OR: 0.037, 95%CI: 0.011-0.119).</p><p><strong>Conclusions: </strong>BPB could decrease the intraoperative pain and improve the 12-month primary patency rates compared with LA for patients underwent PTA treatment of dysfunctional AVF.</p>\",\"PeriodicalId\":20839,\"journal\":{\"name\":\"Renal Failure\",\"volume\":\"47 1\",\"pages\":\"2477834\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915726/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Renal Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/0886022X.2025.2477834\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2025.2477834","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:比较超声引导下臂丛神经阻滞(BPB)与局部麻醉(LA)在经皮腔内血管成形术(PTA)治疗功能失调性动静脉瘘(AVF)的疗效、安全性和12个月通畅率。方法:纳入2021年1月至2022年12月连续接受PTA治疗的功能失调AVF患者。进行重叠加权以调整两组之间的显著差异。主要疗效指标包括视觉模拟评分(VAS)评分和12个月靶病变原发通畅率。次要疗效指标包括目标病变原发辅助通畅率、二次通畅率、通路血栓形成率、通路再干预率和12个月内再干预次数。采用单因素分析和对数二项回归的多因素分析来确定与术中疼痛相关的独立因素。结果:218例患者纳入研究,其中82例患者在BPB下行PTA, 136例患者在LA下行PTA。重叠加权后,两组的基线、病变特征及术中细节无显著差异。BPB组VAS评分明显低于LA组(2.4±1.4 vs 5.1±1.9,p p = 0.037)。BPB组12个月目标病灶一期辅助通畅率和通路二次通畅率均显著高于LA组(p = 0.023和p = 0.028)。BPB组通路血栓形成率(10.0%)明显低于LA组(28.3%)(p = 0.011)。结论:与LA相比,经PTA治疗功能不全AVF的患者,BPB可减轻术中疼痛,提高12个月初通畅率。
Brachial plexus block versus local anesthesia for percutaneous transluminal angioplasty of dysfunctional arteriovenous fistula: 12-month results of a propensity score weighted study.
Objective: The study aimed to compare ultrasound-guided brachial plexus block (BPB) with local anesthesia (LA) on efficacy, safety and 12-month patency rate for percutaneous transluminal angioplasty (PTA) treatment of dysfunctional arteriovenous fistula (AVF).
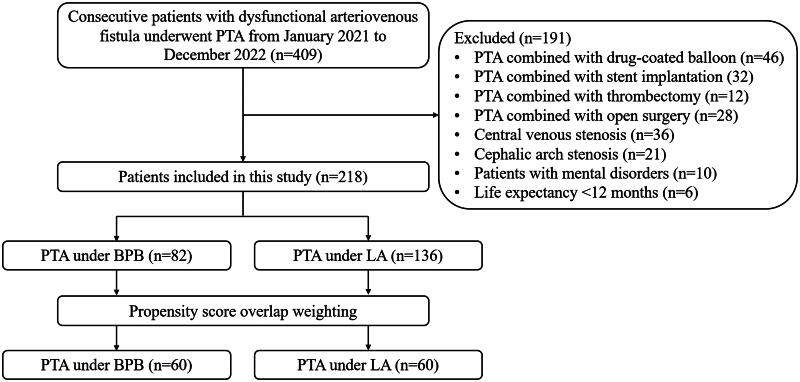
Methods: Consecutive patients with dysfunctional AVF who underwent PTA from January 2021 to December 2022 were included. Overlap weighting was performed to adjust for significant differences between the two groups. The primary efficacy outcomes included visual analogue scale (VAS) score and 12-month target-lesion primary patency rate. The secondary efficacy outcomes included target-lesion primary-assisted patency rate, secondary patency rate, access-circuit thrombosis rate, access-circuit reintervention rate, and number of reinterventions within 12 months. Univariate analysis and multivariate analysis by log-binomial regression were used to identify the independent factors associated with intraoperative pain.
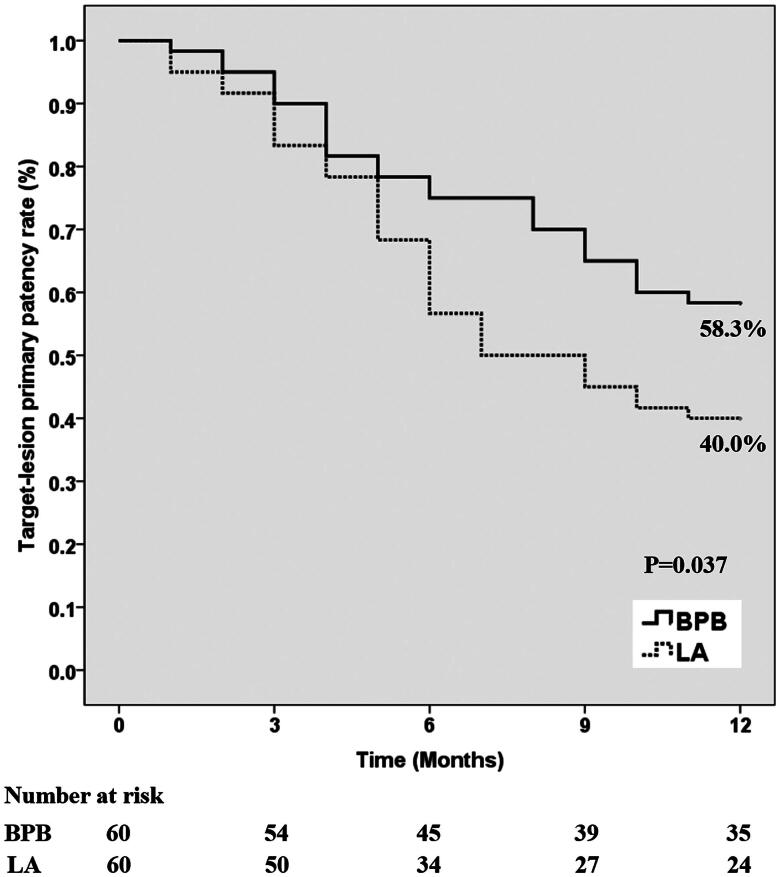
Results: 218 patients were included in the study: 82 patients underwent PTA under BPB and 136 patients underwent PTA under LA. After overlap weighting, the baseline, lesion characteristics and intraoperative details had no significant difference between the two groups. Patients under BPB had significantly lower VAS scores than those under LA (2.4 ± 1.4 vs 5.1 ± 1.9, p < 0.001). The 12-month target-lesion primary patency rate was significantly higher in the BPB group than that in the LA group (58.3% vs 40.0%, p = 0.037). The 12-month target-lesion primary-assisted patency rate and access-circuit secondary patency rate were significantly higher in the BPB group than those in the LA group (p = 0.023 and p = 0.028). The access-circuit thrombosis rate was significantly lower in the BPB group (10.0%) than that in the LA group (28.3%) (p = 0.011). BPB was the only independent factor associated with mild pain (p < 0.001, OR: 0.037, 95%CI: 0.011-0.119).
Conclusions: BPB could decrease the intraoperative pain and improve the 12-month primary patency rates compared with LA for patients underwent PTA treatment of dysfunctional AVF.
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


