Bangsheng Hu, Junsheng Chen, Shuai Han, Zeping Dai, Ju Gao
{"title":"氯吡格雷在腹部手术中的管理:低分子肝素桥接、不桥接和氯吡格雷继续策略围手术期出血风险的比较。","authors":"Bangsheng Hu, Junsheng Chen, Shuai Han, Zeping Dai, Ju Gao","doi":"10.1177/10760296251327594","DOIUrl":null,"url":null,"abstract":"<p><p>Clopidogrel is usually discontinued 5-7 days before elective surgery to reduce the risk of bleeding. However, the perioperative safety of patients receiving low-molecular-weight heparin (LMWH) bridging therapy or continuing clopidogrel therapy remains unknown. We identified patients who received clopidogrel for cardiovascular diseases and underwent elective surgery at a large central hospital in China between June 2022 and January 2024. The primary endpoints were perioperative blood transfusion events and bleeding-related reoperations. A total of 62 patients who received clopidogrel and underwent abdominal surgery were included in this study. Based on the preoperative clopidogrel therapy strategy, patients were categorised into three groups: the LMWH bridging group (clopidogrel withdrawal followed by LMWH bridging therapy for 5-7 days; n = 22), the no-bridging group (clopidogrel withdrawal for 5-7 days; n = 26), and the continued group (clopidogrel therapy maintained; n = 24). Perioperative blood transfusion rates were higher in the LMWH bridging and continued groups. However, there was not a significant distinction (<i>P </i>= .197). Additionally, hospital stay length, bleeding-related reoperation, and 3-month mortality were similar across the groups <i>(P </i>> .05). No patients experienced myocardial infarction or stroke within 3 months post-procedure. Patients who received preoperative LMWH bridging therapy or continued clopidogrel therapy had a slightly higher risk of perioperative bleeding. These findings need to be confirmed by further randomised controlled trials.</p>","PeriodicalId":10335,"journal":{"name":"Clinical and Applied Thrombosis/Hemostasis","volume":"31 ","pages":"10760296251327594"},"PeriodicalIF":2.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915241/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clopidogrel Management in Abdominal Surgery: A Comparison of Perioperative Bleeding Risks with Low-Molecular-Weight Heparin Bridging, No-Bridging and Clopidogrel Continuation Strategies.\",\"authors\":\"Bangsheng Hu, Junsheng Chen, Shuai Han, Zeping Dai, Ju Gao\",\"doi\":\"10.1177/10760296251327594\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Clopidogrel is usually discontinued 5-7 days before elective surgery to reduce the risk of bleeding. However, the perioperative safety of patients receiving low-molecular-weight heparin (LMWH) bridging therapy or continuing clopidogrel therapy remains unknown. We identified patients who received clopidogrel for cardiovascular diseases and underwent elective surgery at a large central hospital in China between June 2022 and January 2024. The primary endpoints were perioperative blood transfusion events and bleeding-related reoperations. A total of 62 patients who received clopidogrel and underwent abdominal surgery were included in this study. Based on the preoperative clopidogrel therapy strategy, patients were categorised into three groups: the LMWH bridging group (clopidogrel withdrawal followed by LMWH bridging therapy for 5-7 days; n = 22), the no-bridging group (clopidogrel withdrawal for 5-7 days; n = 26), and the continued group (clopidogrel therapy maintained; n = 24). Perioperative blood transfusion rates were higher in the LMWH bridging and continued groups. However, there was not a significant distinction (<i>P </i>= .197). Additionally, hospital stay length, bleeding-related reoperation, and 3-month mortality were similar across the groups <i>(P </i>> .05). No patients experienced myocardial infarction or stroke within 3 months post-procedure. Patients who received preoperative LMWH bridging therapy or continued clopidogrel therapy had a slightly higher risk of perioperative bleeding. These findings need to be confirmed by further randomised controlled trials.</p>\",\"PeriodicalId\":10335,\"journal\":{\"name\":\"Clinical and Applied Thrombosis/Hemostasis\",\"volume\":\"31 \",\"pages\":\"10760296251327594\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11915241/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Applied Thrombosis/Hemostasis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/10760296251327594\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Applied Thrombosis/Hemostasis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/10760296251327594","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Clopidogrel Management in Abdominal Surgery: A Comparison of Perioperative Bleeding Risks with Low-Molecular-Weight Heparin Bridging, No-Bridging and Clopidogrel Continuation Strategies.
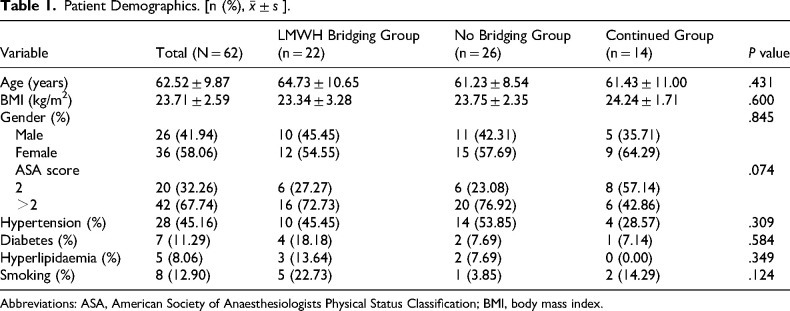
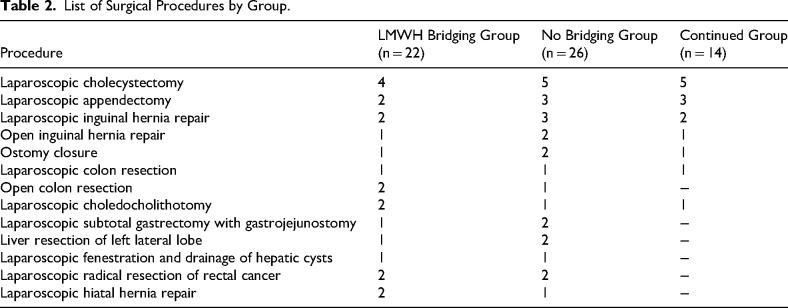
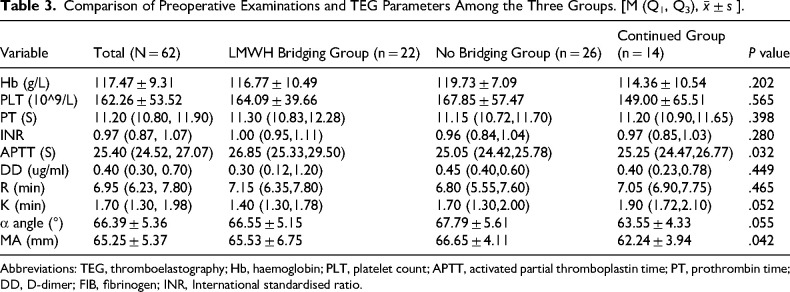
Clopidogrel is usually discontinued 5-7 days before elective surgery to reduce the risk of bleeding. However, the perioperative safety of patients receiving low-molecular-weight heparin (LMWH) bridging therapy or continuing clopidogrel therapy remains unknown. We identified patients who received clopidogrel for cardiovascular diseases and underwent elective surgery at a large central hospital in China between June 2022 and January 2024. The primary endpoints were perioperative blood transfusion events and bleeding-related reoperations. A total of 62 patients who received clopidogrel and underwent abdominal surgery were included in this study. Based on the preoperative clopidogrel therapy strategy, patients were categorised into three groups: the LMWH bridging group (clopidogrel withdrawal followed by LMWH bridging therapy for 5-7 days; n = 22), the no-bridging group (clopidogrel withdrawal for 5-7 days; n = 26), and the continued group (clopidogrel therapy maintained; n = 24). Perioperative blood transfusion rates were higher in the LMWH bridging and continued groups. However, there was not a significant distinction (P = .197). Additionally, hospital stay length, bleeding-related reoperation, and 3-month mortality were similar across the groups (P > .05). No patients experienced myocardial infarction or stroke within 3 months post-procedure. Patients who received preoperative LMWH bridging therapy or continued clopidogrel therapy had a slightly higher risk of perioperative bleeding. These findings need to be confirmed by further randomised controlled trials.
期刊介绍:
CATH is a peer-reviewed bi-monthly journal that addresses the practical clinical and laboratory issues involved in managing bleeding and clotting disorders, especially those related to thrombosis, hemostasis, and vascular disorders. CATH covers clinical trials, studies on etiology, pathophysiology, diagnosis and treatment of thrombohemorrhagic disorders.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


