Allan Klitgaard, Rikke Ibsen, Ole Hilberg, Anders Løkke
{"title":"慢性阻塞性肺疾病患者肺炎风险的城乡差异:一项全国性的基于登记的研究","authors":"Allan Klitgaard, Rikke Ibsen, Ole Hilberg, Anders Løkke","doi":"10.1080/20018525.2025.2477386","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Urban-rural differences in treatment within chronic obstructive pulmonary disease (COPD) have been documented in Denmark, and we aim to investigate such differences in the risk of pneumonia.</p><p><strong>Methods: </strong>A Danish register-based cross-sectional study including patients with an International Classification of Diseases 10<sup>th</sup> revision (ICD-10) diagnosis code of COPD (J.44) alive on the 31st of December 2018 (99,057 patients). Patients were grouped by municipality type on an urban-rural gradient (capital, metropolitan, provincial, commuter, rural). We identified outpatient pneumonias (redeemed prescriptions of antibiotics typically used for pneumonia) and pneumonia hospitalizations (ICD-10 codes) during 2018. Three groups were defined: 1) No pneumonia, 2) at least one outpatient pneumonia (but no pneumonia hospitalization), and 3) at least one pneumonia hospitalization. A multivariable multinomial logistic regression model was performed with municipality type as main explanatory variable. The 'No pneumonia' group was used as reference outcome group.</p><p><strong>Results: </strong>Patients outside capital municipalities had significantly increased risk of experiencing outpatient pneumonia (Metropolitan: Odds ratio (OR) = 1.32, 95% confidence interval (CI): 1.25-1.39. Provincial: OR = 1.26, 95% CI: 1.21-1.31. Commuter: OR = 1.25, 95% CI: 1.20-1.31. Rural: OR = 1.28, 95% CI: 1.23-1.33). No significant differences were found for pneumonia hospitalization.</p><p><strong>Conclusions: </strong>Compared to patients in capital municipalities, patients with a hospital-registered COPD diagnosis in non-capital municipalities had a higher risk of annually redeeming at least one prescription for antibiotics typically used for outpatient pneumonia. We were unable to detect differences in pneumonia hospitalization between municipality types. Our study was not designed to assess causality, and we stress the need for future research to provide actionable insights for health policy makers.</p>","PeriodicalId":11872,"journal":{"name":"European Clinical Respiratory Journal","volume":"12 1","pages":"2477386"},"PeriodicalIF":1.4000,"publicationDate":"2025-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11912242/pdf/","citationCount":"0","resultStr":"{\"title\":\"Urban-rural differences in pneumonia risk in patients with chronic obstructive pulmonary disease: a nationwide register-based study.\",\"authors\":\"Allan Klitgaard, Rikke Ibsen, Ole Hilberg, Anders Løkke\",\"doi\":\"10.1080/20018525.2025.2477386\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Urban-rural differences in treatment within chronic obstructive pulmonary disease (COPD) have been documented in Denmark, and we aim to investigate such differences in the risk of pneumonia.</p><p><strong>Methods: </strong>A Danish register-based cross-sectional study including patients with an International Classification of Diseases 10<sup>th</sup> revision (ICD-10) diagnosis code of COPD (J.44) alive on the 31st of December 2018 (99,057 patients). Patients were grouped by municipality type on an urban-rural gradient (capital, metropolitan, provincial, commuter, rural). We identified outpatient pneumonias (redeemed prescriptions of antibiotics typically used for pneumonia) and pneumonia hospitalizations (ICD-10 codes) during 2018. Three groups were defined: 1) No pneumonia, 2) at least one outpatient pneumonia (but no pneumonia hospitalization), and 3) at least one pneumonia hospitalization. A multivariable multinomial logistic regression model was performed with municipality type as main explanatory variable. The 'No pneumonia' group was used as reference outcome group.</p><p><strong>Results: </strong>Patients outside capital municipalities had significantly increased risk of experiencing outpatient pneumonia (Metropolitan: Odds ratio (OR) = 1.32, 95% confidence interval (CI): 1.25-1.39. Provincial: OR = 1.26, 95% CI: 1.21-1.31. Commuter: OR = 1.25, 95% CI: 1.20-1.31. Rural: OR = 1.28, 95% CI: 1.23-1.33). No significant differences were found for pneumonia hospitalization.</p><p><strong>Conclusions: </strong>Compared to patients in capital municipalities, patients with a hospital-registered COPD diagnosis in non-capital municipalities had a higher risk of annually redeeming at least one prescription for antibiotics typically used for outpatient pneumonia. We were unable to detect differences in pneumonia hospitalization between municipality types. Our study was not designed to assess causality, and we stress the need for future research to provide actionable insights for health policy makers.</p>\",\"PeriodicalId\":11872,\"journal\":{\"name\":\"European Clinical Respiratory Journal\",\"volume\":\"12 1\",\"pages\":\"2477386\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-03-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11912242/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Clinical Respiratory Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1080/20018525.2025.2477386\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Clinical Respiratory Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1080/20018525.2025.2477386","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
Urban-rural differences in pneumonia risk in patients with chronic obstructive pulmonary disease: a nationwide register-based study.
Background: Urban-rural differences in treatment within chronic obstructive pulmonary disease (COPD) have been documented in Denmark, and we aim to investigate such differences in the risk of pneumonia.
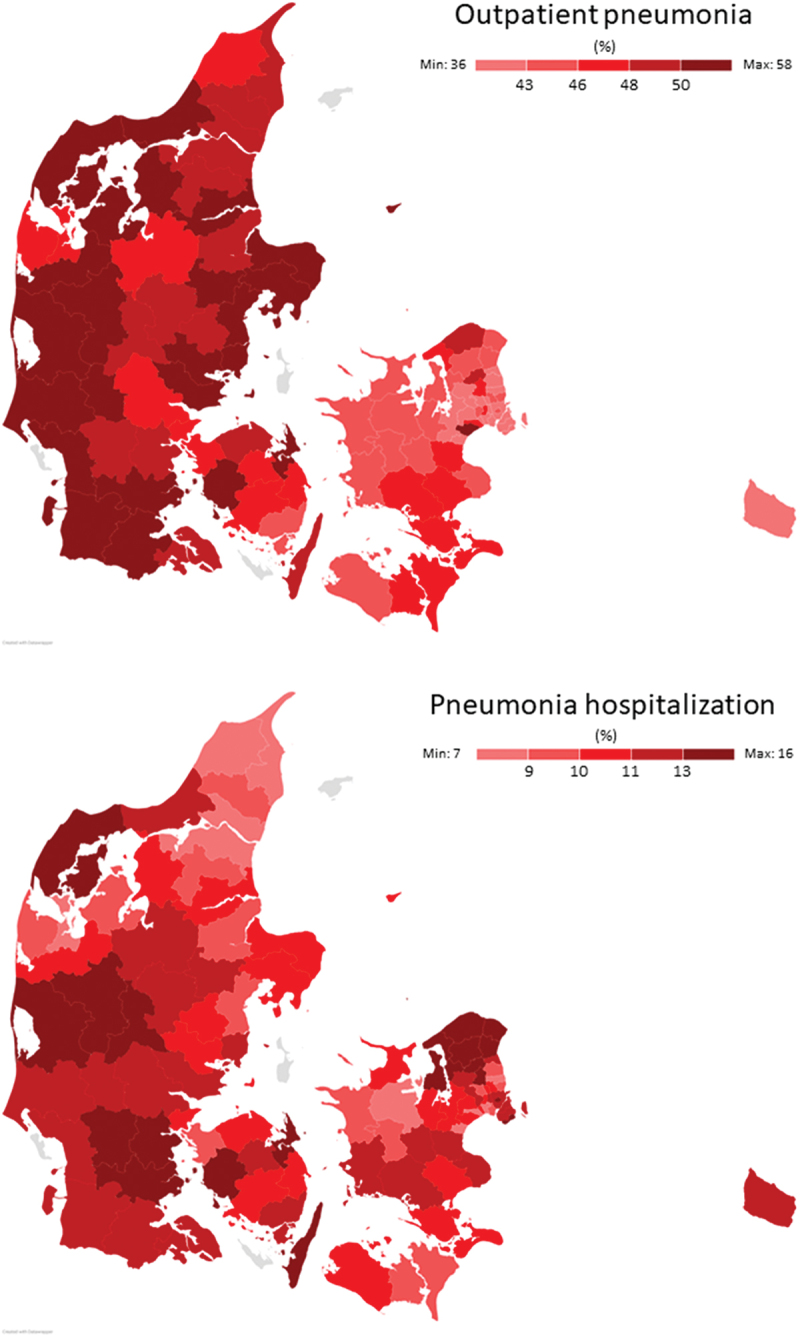
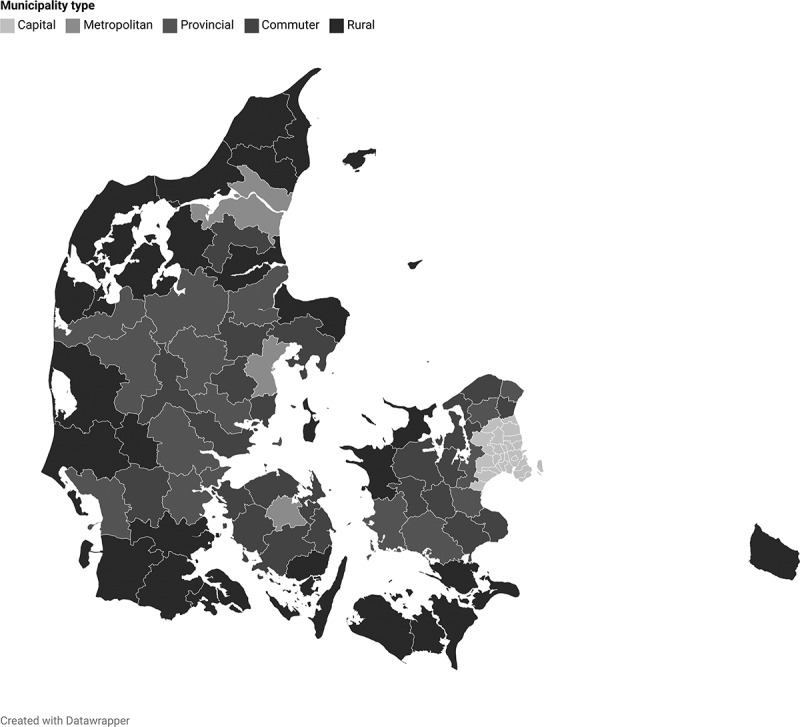
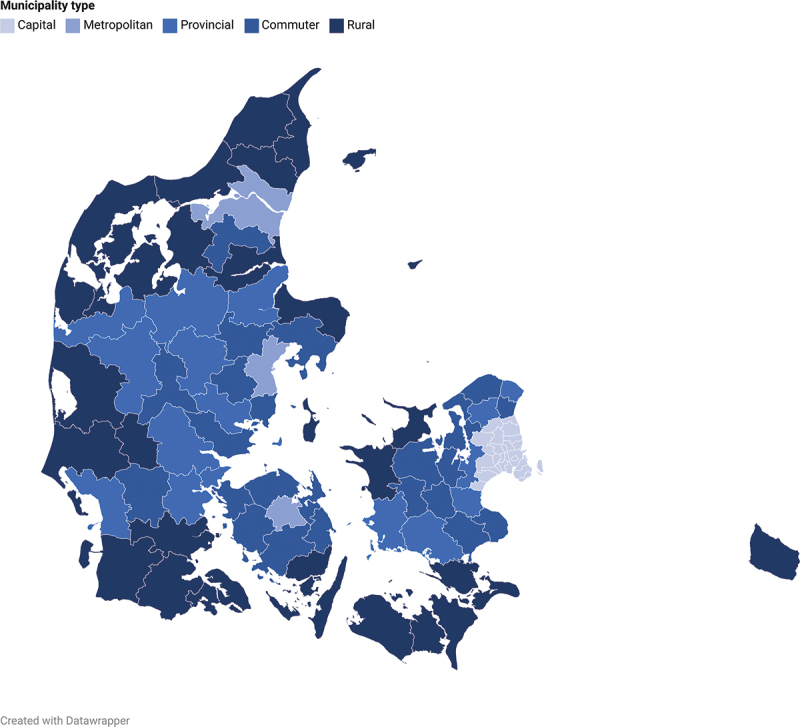
Methods: A Danish register-based cross-sectional study including patients with an International Classification of Diseases 10th revision (ICD-10) diagnosis code of COPD (J.44) alive on the 31st of December 2018 (99,057 patients). Patients were grouped by municipality type on an urban-rural gradient (capital, metropolitan, provincial, commuter, rural). We identified outpatient pneumonias (redeemed prescriptions of antibiotics typically used for pneumonia) and pneumonia hospitalizations (ICD-10 codes) during 2018. Three groups were defined: 1) No pneumonia, 2) at least one outpatient pneumonia (but no pneumonia hospitalization), and 3) at least one pneumonia hospitalization. A multivariable multinomial logistic regression model was performed with municipality type as main explanatory variable. The 'No pneumonia' group was used as reference outcome group.
Results: Patients outside capital municipalities had significantly increased risk of experiencing outpatient pneumonia (Metropolitan: Odds ratio (OR) = 1.32, 95% confidence interval (CI): 1.25-1.39. Provincial: OR = 1.26, 95% CI: 1.21-1.31. Commuter: OR = 1.25, 95% CI: 1.20-1.31. Rural: OR = 1.28, 95% CI: 1.23-1.33). No significant differences were found for pneumonia hospitalization.
Conclusions: Compared to patients in capital municipalities, patients with a hospital-registered COPD diagnosis in non-capital municipalities had a higher risk of annually redeeming at least one prescription for antibiotics typically used for outpatient pneumonia. We were unable to detect differences in pneumonia hospitalization between municipality types. Our study was not designed to assess causality, and we stress the need for future research to provide actionable insights for health policy makers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


