Wissam Harmouch, Ravi Thakker, Alexander Dang, Abdelazeem Mohamed Etewa, Krishna Suthar, Salim Hayek, Wissam Khalife, Ayman Elbadawi
{"title":"ACEi和ARBs作为蒽环类药物化疗患者癌症治疗相关心肌病的一级预防:系统回顾和荟萃分析","authors":"Wissam Harmouch, Ravi Thakker, Alexander Dang, Abdelazeem Mohamed Etewa, Krishna Suthar, Salim Hayek, Wissam Khalife, Ayman Elbadawi","doi":"10.1007/s40119-025-00401-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Anthracyclines treat a myriad of malignancies; however, they are known to lead to cancer therapy-related cardiomyopathy (CTRC). Randomized controlled trials (RCTs) evaluating the role of angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) in primary prevention of CTRC have yielded mixed results.</p><p><strong>Methods: </strong>A systematic search of MEDLINE, Cochrane, and Scopus databases was performed to identify RCTs that evaluated outcomes in patients receiving anthracyclines and ACEi or ARBs versus control. The primary outcome was occurrence of CTRC. All data were pooled using a random-effects model.</p><p><strong>Results: </strong>The final analysis included 10 RCTs, with 1049 patients assessed. The weighted follow-up period was 16.8 months. The average age was 43.2 years and 90% were female. Breast cancer (80%) and lymphomas (13%) were the most common malignancies. There was no statistically significant difference between the groups with regards to occurrence of CTRC (16% vs 24%; risk ratio (RR) 0.67, 95% confidence interval (CI) [0.31, 1.45]). Compared with control, ACEi/ARBs were associated with favorable absolute changes in left ventricular ejection fraction (LVEF) (standardized mean difference (SMD) + 1.20%, 95% CI [0.40, 2.00]), left ventricular end-diastolic volume (SMD - 0.36 mL, 95% CI [- 0.66, - 0.06]), and left ventricular end-systolic volume (SMD - 1.04 mL, 95% CI [- 1.79, - 0.29]). There was also a lower risk of arrhythmias in the ACEi/ARBs group compared to control (1.6% vs 8.0%; RR 0.30, 95% CI [0.10, 0.94]), but no difference in all-cause mortality (2.8% vs 3.2%; RR 0.82, 95% CI [0.26, 2.61]), or heart failure (1.2% vs 7.1%; RR 0.40, 95% CI [0.03, 4.54]).</p><p><strong>Conclusions: </strong>ACEi/ARBs therapy was not associated with a reduction in CTRC among patients with cancer receiving anthracyclines. However, there were favorable changes in LVEF and left ventricular remodeling with ACEi/ARBs therapy. Further large-scale studies are needed to better understand the potential role of ACEi/ARBs in preventing long-term cardiotoxicity.</p>","PeriodicalId":9561,"journal":{"name":"Cardiology and Therapy","volume":" ","pages":"141-159"},"PeriodicalIF":2.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084476/pdf/","citationCount":"0","resultStr":"{\"title\":\"ACEi and ARBs as Primary Prevention of Cancer Therapy-Related Cardiomyopathy in Patients Undergoing Chemotherapy with Anthracyclines: A Systematic Review and Meta-Analysis.\",\"authors\":\"Wissam Harmouch, Ravi Thakker, Alexander Dang, Abdelazeem Mohamed Etewa, Krishna Suthar, Salim Hayek, Wissam Khalife, Ayman Elbadawi\",\"doi\":\"10.1007/s40119-025-00401-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Anthracyclines treat a myriad of malignancies; however, they are known to lead to cancer therapy-related cardiomyopathy (CTRC). Randomized controlled trials (RCTs) evaluating the role of angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) in primary prevention of CTRC have yielded mixed results.</p><p><strong>Methods: </strong>A systematic search of MEDLINE, Cochrane, and Scopus databases was performed to identify RCTs that evaluated outcomes in patients receiving anthracyclines and ACEi or ARBs versus control. The primary outcome was occurrence of CTRC. All data were pooled using a random-effects model.</p><p><strong>Results: </strong>The final analysis included 10 RCTs, with 1049 patients assessed. The weighted follow-up period was 16.8 months. The average age was 43.2 years and 90% were female. Breast cancer (80%) and lymphomas (13%) were the most common malignancies. There was no statistically significant difference between the groups with regards to occurrence of CTRC (16% vs 24%; risk ratio (RR) 0.67, 95% confidence interval (CI) [0.31, 1.45]). Compared with control, ACEi/ARBs were associated with favorable absolute changes in left ventricular ejection fraction (LVEF) (standardized mean difference (SMD) + 1.20%, 95% CI [0.40, 2.00]), left ventricular end-diastolic volume (SMD - 0.36 mL, 95% CI [- 0.66, - 0.06]), and left ventricular end-systolic volume (SMD - 1.04 mL, 95% CI [- 1.79, - 0.29]). There was also a lower risk of arrhythmias in the ACEi/ARBs group compared to control (1.6% vs 8.0%; RR 0.30, 95% CI [0.10, 0.94]), but no difference in all-cause mortality (2.8% vs 3.2%; RR 0.82, 95% CI [0.26, 2.61]), or heart failure (1.2% vs 7.1%; RR 0.40, 95% CI [0.03, 4.54]).</p><p><strong>Conclusions: </strong>ACEi/ARBs therapy was not associated with a reduction in CTRC among patients with cancer receiving anthracyclines. However, there were favorable changes in LVEF and left ventricular remodeling with ACEi/ARBs therapy. Further large-scale studies are needed to better understand the potential role of ACEi/ARBs in preventing long-term cardiotoxicity.</p>\",\"PeriodicalId\":9561,\"journal\":{\"name\":\"Cardiology and Therapy\",\"volume\":\" \",\"pages\":\"141-159\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084476/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiology and Therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40119-025-00401-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology and Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40119-025-00401-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/16 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
ACEi and ARBs as Primary Prevention of Cancer Therapy-Related Cardiomyopathy in Patients Undergoing Chemotherapy with Anthracyclines: A Systematic Review and Meta-Analysis.
Introduction: Anthracyclines treat a myriad of malignancies; however, they are known to lead to cancer therapy-related cardiomyopathy (CTRC). Randomized controlled trials (RCTs) evaluating the role of angiotensin converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARBs) in primary prevention of CTRC have yielded mixed results.
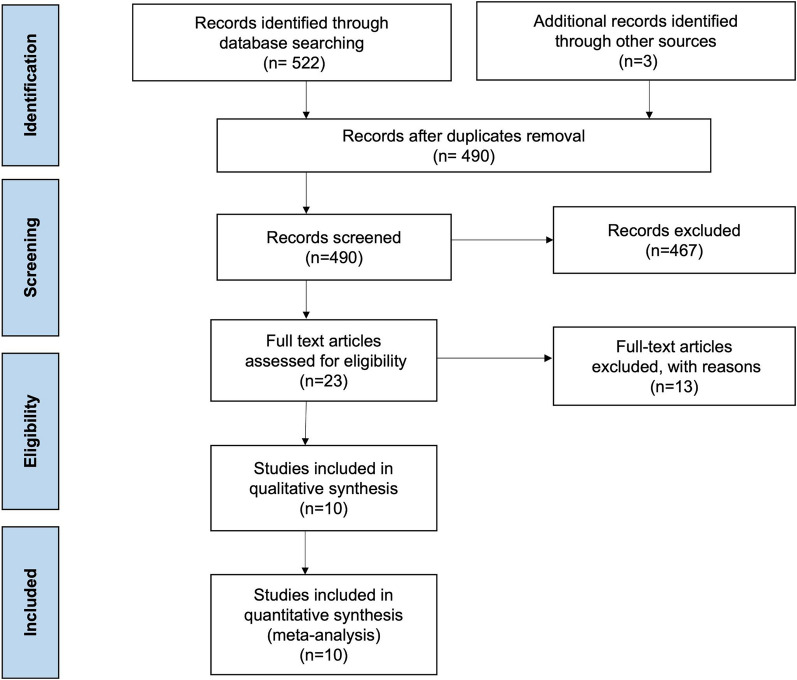
Methods: A systematic search of MEDLINE, Cochrane, and Scopus databases was performed to identify RCTs that evaluated outcomes in patients receiving anthracyclines and ACEi or ARBs versus control. The primary outcome was occurrence of CTRC. All data were pooled using a random-effects model.
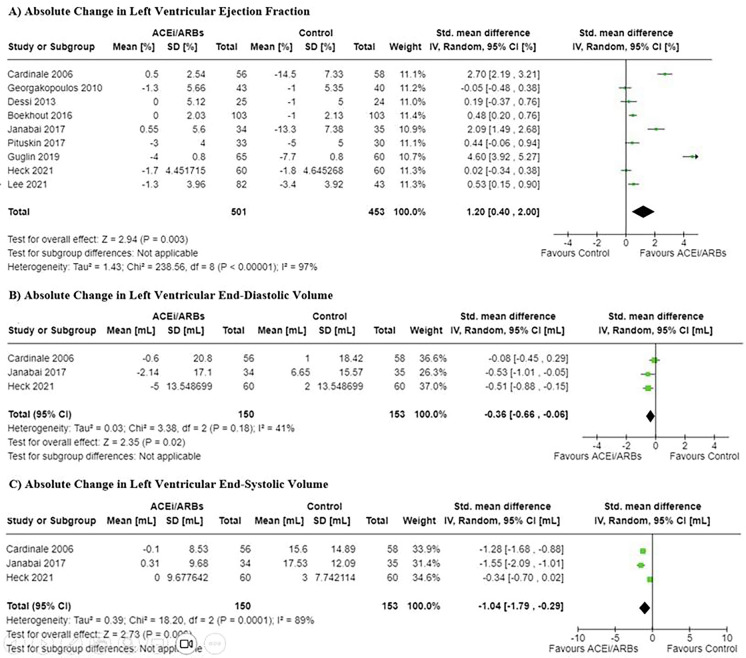
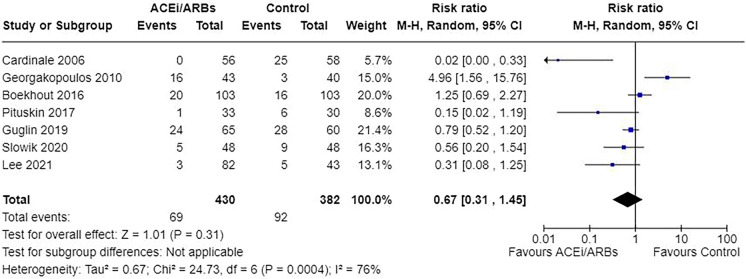
Results: The final analysis included 10 RCTs, with 1049 patients assessed. The weighted follow-up period was 16.8 months. The average age was 43.2 years and 90% were female. Breast cancer (80%) and lymphomas (13%) were the most common malignancies. There was no statistically significant difference between the groups with regards to occurrence of CTRC (16% vs 24%; risk ratio (RR) 0.67, 95% confidence interval (CI) [0.31, 1.45]). Compared with control, ACEi/ARBs were associated with favorable absolute changes in left ventricular ejection fraction (LVEF) (standardized mean difference (SMD) + 1.20%, 95% CI [0.40, 2.00]), left ventricular end-diastolic volume (SMD - 0.36 mL, 95% CI [- 0.66, - 0.06]), and left ventricular end-systolic volume (SMD - 1.04 mL, 95% CI [- 1.79, - 0.29]). There was also a lower risk of arrhythmias in the ACEi/ARBs group compared to control (1.6% vs 8.0%; RR 0.30, 95% CI [0.10, 0.94]), but no difference in all-cause mortality (2.8% vs 3.2%; RR 0.82, 95% CI [0.26, 2.61]), or heart failure (1.2% vs 7.1%; RR 0.40, 95% CI [0.03, 4.54]).
Conclusions: ACEi/ARBs therapy was not associated with a reduction in CTRC among patients with cancer receiving anthracyclines. However, there were favorable changes in LVEF and left ventricular remodeling with ACEi/ARBs therapy. Further large-scale studies are needed to better understand the potential role of ACEi/ARBs in preventing long-term cardiotoxicity.
期刊介绍:
Aims and Scope
Cardiology and Therapy is an international, open access, peer reviewed (single-blind), rapid-publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of cardiovascular therapies and interventions, including devices. Studies relating to diagnosis and diagnostics, pharmacoeconomics, public health, quality of life, as well as patient care, management and education are also encouraged.
Areas of focus include, but are not limited to, ischaemic heart disease and acute cardiac care, myocardial, valvular, pericardial and congenital heart disease, vascular and pulmonary disease (including hypertension), arrhythmias, heart failure, non-invasive diagnostic techniques, and invasive and interventional cardiology as well as cardiovascular surgery.
The journal is of interest to a broad audience of pharmaceutical and healthcare professionals and publishes original research, reviews, case reports/case series, trial protocols and short communications such as commentaries and editorials. Cardiolology and Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of quality research, which may be considered of insufficient interest by other journals.
Rapid Publication
The journal’s publication timelines aim for a rapid peer review of 2 weeks. If an article is accepted it will be published 3–4 weeks from acceptance. The rapid timelines are achieved through the combination of a dedicated in-house editorial team, who manage article workflow, and an extensive Editorial and Advisory Board who assist with peer review. This allows the journal to support the rapid dissemination of research, whilst still providing robust peer review. Combined with the journal’s open access model this allows for the rapid, efficient communication of the latest research and reviews, fostering the advancement of cardiovascular therapies.
Personal Service
The journal’s dedicated in-house editorial team offer a personal “concierge service” meaning authors will always have an editorial contact able to update them on the status of their manuscript. The editorial team check all manuscripts to ensure that articles conform to the most recent COPE, GPP and ICMJE publishing guidelines. This supports the publication of ethically sound and transparent research.
Digital Features and Plain Language Summaries
Cardiology and Therapy offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by key summary points, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article. The journal also provides the option to include various types of digital features including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations. All additional features are peer reviewed to the same high standard as the article itself. If you consider that your paper would benefit from the inclusion of a digital feature, please let us know. Our editorial team are able to create high-quality slide decks and infographics in-house, and video abstracts through our partner Research Square, and would be happy to assist in any way we can. For further information about digital features, please contact the journal editor (see ‘Contact the Journal’ for email address), and see the ‘Guidelines for digital features and plain language summaries’ document under ‘Submission guidelines’.
For examples of digital features please visit our showcase page https://springerhealthcare.com/expertise/publishing-digital-features/
Publication Fees
Upon acceptance of your article for publication, authors will be required to pay the mandatory Rapid Service Fee of £3650/€4500/$5100. The journal will consider fee discounts for developing countries and this is decided on a case by case basis.
Open Access
All articles published by Cardiology and Therapy are published open access.
Peer Review Process
Upon submission, manuscripts are assessed by the editorial team to ensure they fit within the aims and scope of the journal and are also checked for plagiarism. All suitable submissions are then subject to a comprehensive single-blind peer review. Reviewers are selected based on their relevant expertise and publication history in the subject area. The journal has an extensive pool of editorial and advisory board members who have been selected to assist with peer review based on the afore-mentioned criteria.
At least two extensive reviews are required to make the editorial decision, with the exception of some article types such as Commentaries, Editorials and Letters which are generally reviewed by one member of the Editorial Board. Where reviewer recommendations are conflicted, the editorial board will be contacted for further advice and a presiding decision. Manuscripts are then either accepted, rejected or authors are required to make major or minor revisions (both reviewer comments and editorial comments may need to be addressed). Once a revised manuscript is re-submitted, it is assessed along with the responses to reviewer comments and if it has been adequately revised it will be accepted for publication. Accepted manuscripts are then copyedited and typeset by the production team before online publication. Appeals against decisions following peer review are considered on a case by case basis and should be sent to the journal editor.
Preprints
We encourage posting of preprints of primary research manuscripts on preprint servers, authors’ or institutional websites, and open communications between researchers whether on community preprint servers or preprint commenting platforms. Posting of preprints is not considered prior publication and will not jeopardize consideration in our journals. Authors should disclose details of preprint posting during the submission process or at any other point during consideration in one of our journals. Once the preprint is published, it is the author’s responsibility to ensure that the preprint record is updated with a publication reference, including the DOI and a URL link to the published version of the article on the journal website.
Copyright
Cardiology and Therapy is published under the Creative Commons Attribution-Noncommercial License, which allows users to read, copy, distribute, and make derivative works for non-commercial purposes from the material, as long as the author of the original work is cited. The author assigns the exclusive right to any commercial use of the article to Springer. For more information about the Creative Commons Attribution-Noncommercial License, click here: http://creativecommons.org/licenses/by-nc/4.0.
Contact
For more information about the journal, including pre-submission enquiries, please contact matthew.evans@springer.com

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


