Phyu Sin Aye, Joanne Barnes, George Laking, Laird Cameron, Malcolm Anderson, Brendan Luey, Stephen Delany, Dean Harris, Blair McLaren, Elliott Brenman, Jayden Wong, Ross Lawrenson, Michael Arendse, Sandar Tin Tin, Mark Elwood, Philip Hope, Mark James McKeage
{"title":"2010年至2020年,厄洛替尼和吉非替尼治疗新西兰Aotearoa地区晚期表皮生长因子受体突变的非鳞状非小细胞肺癌的治疗结果:全国全患者人群回顾性队列研究","authors":"Phyu Sin Aye, Joanne Barnes, George Laking, Laird Cameron, Malcolm Anderson, Brendan Luey, Stephen Delany, Dean Harris, Blair McLaren, Elliott Brenman, Jayden Wong, Ross Lawrenson, Michael Arendse, Sandar Tin Tin, Mark Elwood, Philip Hope, Mark James McKeage","doi":"10.2196/65118","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Health care system-wide outcomes from routine treatment with erlotinib and gefitinib are incompletely understood.</p><p><strong>Objective: </strong>The aim of the study is to describe the effectiveness of erlotinib and gefitinib during the first decade of their routine use for treating advanced epidermal growth factor receptor (EGFR) mutation-positive nonsquamous non-small cell lung cancer in the entire cohort of patients treated in Aotearoa New Zealand.</p><p><strong>Methods: </strong>Patients were identified, and data collated from national pharmaceutical dispensing, cancer registration, and mortality registration electronic databases by deterministic data linkage using National Health Index numbers. Time-to-treatment discontinuation and overall survival were measured from the date of first dispensing of erlotinib or gefitinib and analyzed by Kaplan-Meier curves. Associations of treatment outcomes with baseline factors were evaluated using univariable and multivariable Cox regressions.</p><p><strong>Results: </strong>Overall, 752 patients were included who started treatment with erlotinib (n=418) or gefitinib (n=334) before October 2020. Median time-to-treatment discontinuation was 11.6 (95% CI 10.8-12.4) months, and median overall survival was 20.1 (95% CI 18.1-21.6) months. Shorter time-to-treatment discontinuation was independently associated with high socioeconomic deprivation (hazard ratio [HR] 1.3, 95% CI 1.1-1.5 compared to the New Zealand Index of Deprivation 1-4 group), EGFR L858R mutations (HR 1.3, 95% CI 1.1-1.6 compared to exon 19 deletion), and distant disease at cancer diagnosis (HR 1.4, 95% CI 1.2-1.7 compared to localized or regional disease). The same factors were independently associated with shorter overall survival. Outcome estimates and predictors remained unchanged in sensitivity analyses.</p><p><strong>Conclusions: </strong>Outcomes from routine treatment with erlotinib and gefitinib in New Zealand patients with advanced EGFR-mutant nonsquamous non-small cell lung cancer are comparable with those reported in randomized trials and other health care system-wide retrospective cohort studies. Socioeconomic status, EGFR mutation subtype, and disease extent at cancer diagnosis were independent predictors of treatment outcomes in that setting.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"11 ","pages":"e65118"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11892703/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment Outcomes From Erlotinib and Gefitinib in Advanced Epidermal Growth Factor Receptor-Mutated Nonsquamous Non-Small Cell Lung Cancer in Aotearoa New Zealand From 2010 to 2020: Nationwide Whole-of-Patient-Population Retrospective Cohort Study.\",\"authors\":\"Phyu Sin Aye, Joanne Barnes, George Laking, Laird Cameron, Malcolm Anderson, Brendan Luey, Stephen Delany, Dean Harris, Blair McLaren, Elliott Brenman, Jayden Wong, Ross Lawrenson, Michael Arendse, Sandar Tin Tin, Mark Elwood, Philip Hope, Mark James McKeage\",\"doi\":\"10.2196/65118\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Health care system-wide outcomes from routine treatment with erlotinib and gefitinib are incompletely understood.</p><p><strong>Objective: </strong>The aim of the study is to describe the effectiveness of erlotinib and gefitinib during the first decade of their routine use for treating advanced epidermal growth factor receptor (EGFR) mutation-positive nonsquamous non-small cell lung cancer in the entire cohort of patients treated in Aotearoa New Zealand.</p><p><strong>Methods: </strong>Patients were identified, and data collated from national pharmaceutical dispensing, cancer registration, and mortality registration electronic databases by deterministic data linkage using National Health Index numbers. Time-to-treatment discontinuation and overall survival were measured from the date of first dispensing of erlotinib or gefitinib and analyzed by Kaplan-Meier curves. Associations of treatment outcomes with baseline factors were evaluated using univariable and multivariable Cox regressions.</p><p><strong>Results: </strong>Overall, 752 patients were included who started treatment with erlotinib (n=418) or gefitinib (n=334) before October 2020. Median time-to-treatment discontinuation was 11.6 (95% CI 10.8-12.4) months, and median overall survival was 20.1 (95% CI 18.1-21.6) months. Shorter time-to-treatment discontinuation was independently associated with high socioeconomic deprivation (hazard ratio [HR] 1.3, 95% CI 1.1-1.5 compared to the New Zealand Index of Deprivation 1-4 group), EGFR L858R mutations (HR 1.3, 95% CI 1.1-1.6 compared to exon 19 deletion), and distant disease at cancer diagnosis (HR 1.4, 95% CI 1.2-1.7 compared to localized or regional disease). The same factors were independently associated with shorter overall survival. Outcome estimates and predictors remained unchanged in sensitivity analyses.</p><p><strong>Conclusions: </strong>Outcomes from routine treatment with erlotinib and gefitinib in New Zealand patients with advanced EGFR-mutant nonsquamous non-small cell lung cancer are comparable with those reported in randomized trials and other health care system-wide retrospective cohort studies. Socioeconomic status, EGFR mutation subtype, and disease extent at cancer diagnosis were independent predictors of treatment outcomes in that setting.</p>\",\"PeriodicalId\":45538,\"journal\":{\"name\":\"JMIR Cancer\",\"volume\":\"11 \",\"pages\":\"e65118\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-03-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11892703/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMIR Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/65118\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/65118","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:卫生保健系统范围内厄洛替尼和吉非替尼常规治疗的结果尚不完全清楚。目的:本研究的目的是描述厄洛替尼和吉非替尼在第一个十年常规使用治疗晚期表皮生长因子受体(EGFR)突变阳性的非鳞状非小细胞肺癌在新西兰Aotearoa治疗的整个队列患者的有效性。方法:采用确定性数据链接,利用国家健康指数编号对国家药品调剂、癌症登记和死亡登记电子数据库中的患者进行识别和数据整理。从首次配药厄洛替尼或吉非替尼开始测量停药时间和总生存期,并通过Kaplan-Meier曲线进行分析。使用单变量和多变量Cox回归评估治疗结果与基线因素的相关性。结果:总体而言,752名患者在2020年10月之前开始接受厄洛替尼(n=418)或吉非替尼(n=334)治疗。中位停药时间为11.6个月(95% CI 10.8-12.4),中位总生存期为20.1个月(95% CI 18.1-21.6)。较短的停药时间与较高的社会经济剥夺(风险比[HR] 1.3, 95% CI 1.1-1.5,与新西兰剥夺指数1-4组相比)、EGFR L858R突变(风险比[HR] 1.3, 95% CI 1.1-1.6,与外显子19缺失相比)和癌症诊断时的远处疾病(风险比1.4,95% CI 1.2-1.7,与局部或区域性疾病相比)独立相关。同样的因素与较短的总生存期独立相关。敏感性分析的结果估计和预测因子保持不变。结论:厄洛替尼和吉非替尼常规治疗新西兰晚期egfr突变非鳞状非小细胞肺癌患者的结果与随机试验和其他卫生保健系统回顾性队列研究报告的结果相当。在这种情况下,社会经济地位、EGFR突变亚型和癌症诊断时的疾病程度是治疗结果的独立预测因素。
Treatment Outcomes From Erlotinib and Gefitinib in Advanced Epidermal Growth Factor Receptor-Mutated Nonsquamous Non-Small Cell Lung Cancer in Aotearoa New Zealand From 2010 to 2020: Nationwide Whole-of-Patient-Population Retrospective Cohort Study.
Background: Health care system-wide outcomes from routine treatment with erlotinib and gefitinib are incompletely understood.
Objective: The aim of the study is to describe the effectiveness of erlotinib and gefitinib during the first decade of their routine use for treating advanced epidermal growth factor receptor (EGFR) mutation-positive nonsquamous non-small cell lung cancer in the entire cohort of patients treated in Aotearoa New Zealand.
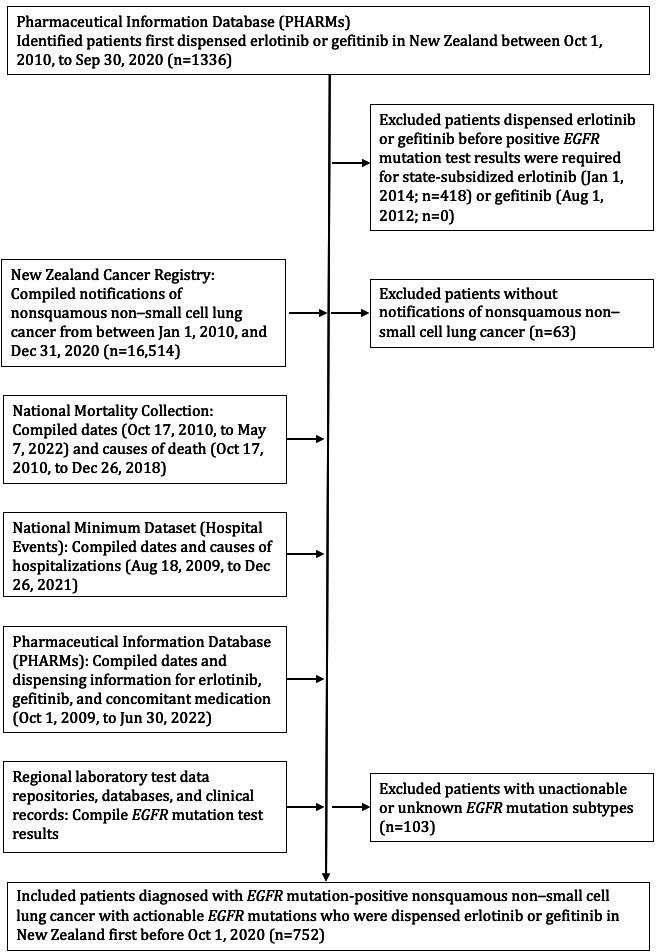
Methods: Patients were identified, and data collated from national pharmaceutical dispensing, cancer registration, and mortality registration electronic databases by deterministic data linkage using National Health Index numbers. Time-to-treatment discontinuation and overall survival were measured from the date of first dispensing of erlotinib or gefitinib and analyzed by Kaplan-Meier curves. Associations of treatment outcomes with baseline factors were evaluated using univariable and multivariable Cox regressions.
Results: Overall, 752 patients were included who started treatment with erlotinib (n=418) or gefitinib (n=334) before October 2020. Median time-to-treatment discontinuation was 11.6 (95% CI 10.8-12.4) months, and median overall survival was 20.1 (95% CI 18.1-21.6) months. Shorter time-to-treatment discontinuation was independently associated with high socioeconomic deprivation (hazard ratio [HR] 1.3, 95% CI 1.1-1.5 compared to the New Zealand Index of Deprivation 1-4 group), EGFR L858R mutations (HR 1.3, 95% CI 1.1-1.6 compared to exon 19 deletion), and distant disease at cancer diagnosis (HR 1.4, 95% CI 1.2-1.7 compared to localized or regional disease). The same factors were independently associated with shorter overall survival. Outcome estimates and predictors remained unchanged in sensitivity analyses.
Conclusions: Outcomes from routine treatment with erlotinib and gefitinib in New Zealand patients with advanced EGFR-mutant nonsquamous non-small cell lung cancer are comparable with those reported in randomized trials and other health care system-wide retrospective cohort studies. Socioeconomic status, EGFR mutation subtype, and disease extent at cancer diagnosis were independent predictors of treatment outcomes in that setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


