{"title":"单倍体造血细胞移植治疗先天性角化不良伴骨髓增生异常综合征/急性髓系白血病。","authors":"Sayan Sinha Roy, Manswinee Mallik, Alka Khadwal, Pradeep Kishore Reddy Gogulamudi, Arihant Jain, Gaurav Prakash, Pankaj Malhotra","doi":"10.31547/bct-2024-022","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Allogeneic hematopoietic cell transplantation (Allo-HCT) is the only curative option for marrow failure, myelodysplastic syndrome (MDS), and acute myeloid leukemia associated with dyskeratosis congenita (DKC). Due to chromosomal instability and sensitivity to radiation and alkylating agents, HCT is associated with a high incidence of transplant-related mortality in DKC.</p><p><strong>Case report: </strong>A 25-year-old male presented with DKC-associated cutaneous manifestations and myelodysplastic syndrome / acute myelogenous leukemia (MDS/AML). Targeted next-generation sequencing revealed mutation of the DKC1 and RUNX1 genes. His mother and sibling sisters were carriers for the DKC1 mutation. Due to high donor-specific antibody mean fluorescence intensity (DSA-MFI) against the unshared Human Leukocyte Antigen-A (HLA-A) allele of his 6/12 HLA-matched father, his paternal cousin's sister was selected as a haploidentical (6/12 HLA-matched) donor for HCT. He underwent allo-HCT with stable disease burden using a specifically-designed RIC regimen containing treosulfan (at 50% reduced dosing), fludarabine, and rabbit anti-thymocyte globulin. The graft versus host disease (GVHD) prophylaxis contained reduced-dose post-transplant cyclophosphamide (PTCy dose reduction of 50%) with mycophenolate mofetil and cyclosporine. He engrafted with complete donor chimerism, and the day +30 marrow was in complete morphological remission with undetectable measurable residual disease by flow cytometry. On day +126, he developed steroid-responsive late-onset grade II acute GVHD (stage III skin GVHD). He suffered from morphologic relapse on day +220 and succumbed from sepsis with septic shock on day +256.</p><p><strong>Conclusion: </strong>This case demonstrates the safety and feasibility of haploidentical-HCT using a treosulfan-based reduced-intensity conditioning (RIC) regimen and modified PTCy-based GVHD prophylaxis in DKC. Disease relapse in this patient underscores the impact of pretransplant disease burden on relapse free survival in DKC patients with MDS/AML who are not eligible for myeloablative conditioning.</p>","PeriodicalId":72423,"journal":{"name":"Blood cell therapy","volume":"8 1","pages":"186-189"},"PeriodicalIF":0.0000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11883479/pdf/","citationCount":"0","resultStr":"{\"title\":\"Haploidentical Hematopoietic Cell Transplantation in Dyskeratosis Congenita with Myelodysplastic Syndrome/Acute Myeloid Leukemia.\",\"authors\":\"Sayan Sinha Roy, Manswinee Mallik, Alka Khadwal, Pradeep Kishore Reddy Gogulamudi, Arihant Jain, Gaurav Prakash, Pankaj Malhotra\",\"doi\":\"10.31547/bct-2024-022\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Allogeneic hematopoietic cell transplantation (Allo-HCT) is the only curative option for marrow failure, myelodysplastic syndrome (MDS), and acute myeloid leukemia associated with dyskeratosis congenita (DKC). Due to chromosomal instability and sensitivity to radiation and alkylating agents, HCT is associated with a high incidence of transplant-related mortality in DKC.</p><p><strong>Case report: </strong>A 25-year-old male presented with DKC-associated cutaneous manifestations and myelodysplastic syndrome / acute myelogenous leukemia (MDS/AML). Targeted next-generation sequencing revealed mutation of the DKC1 and RUNX1 genes. His mother and sibling sisters were carriers for the DKC1 mutation. Due to high donor-specific antibody mean fluorescence intensity (DSA-MFI) against the unshared Human Leukocyte Antigen-A (HLA-A) allele of his 6/12 HLA-matched father, his paternal cousin's sister was selected as a haploidentical (6/12 HLA-matched) donor for HCT. He underwent allo-HCT with stable disease burden using a specifically-designed RIC regimen containing treosulfan (at 50% reduced dosing), fludarabine, and rabbit anti-thymocyte globulin. The graft versus host disease (GVHD) prophylaxis contained reduced-dose post-transplant cyclophosphamide (PTCy dose reduction of 50%) with mycophenolate mofetil and cyclosporine. He engrafted with complete donor chimerism, and the day +30 marrow was in complete morphological remission with undetectable measurable residual disease by flow cytometry. On day +126, he developed steroid-responsive late-onset grade II acute GVHD (stage III skin GVHD). He suffered from morphologic relapse on day +220 and succumbed from sepsis with septic shock on day +256.</p><p><strong>Conclusion: </strong>This case demonstrates the safety and feasibility of haploidentical-HCT using a treosulfan-based reduced-intensity conditioning (RIC) regimen and modified PTCy-based GVHD prophylaxis in DKC. Disease relapse in this patient underscores the impact of pretransplant disease burden on relapse free survival in DKC patients with MDS/AML who are not eligible for myeloablative conditioning.</p>\",\"PeriodicalId\":72423,\"journal\":{\"name\":\"Blood cell therapy\",\"volume\":\"8 1\",\"pages\":\"186-189\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-02-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11883479/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood cell therapy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31547/bct-2024-022\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood cell therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31547/bct-2024-022","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:同种异体造血细胞移植(alloo - hct)是治疗骨髓衰竭、骨髓增生异常综合征(MDS)和急性髓系白血病合并先天性角化不良(DKC)的唯一选择。由于染色体不稳定性和对辐射和烷基化剂的敏感性,HCT与DKC中移植相关死亡率的高发生率相关。病例报告:一名25岁男性表现为dkc相关皮肤表现和骨髓增生异常综合征/急性髓性白血病(MDS/AML)。靶向下一代测序显示DKC1和RUNX1基因突变。他的母亲和兄弟姐妹是DKC1突变的携带者。由于其6/12 hla匹配的父亲的非共享人类白细胞抗原- a (HLA-A)等位基因具有较高的供体特异性抗体平均荧光强度(DSA-MFI),因此选择其堂妹作为HCT的单倍体相同(6/12 hla匹配)供体。他接受了同种异体hct治疗,疾病负担稳定,使用了专门设计的RIC方案,其中含有曲硫丹(减少50%剂量)、氟达拉滨和兔抗胸腺细胞球蛋白。移植物抗宿主病(GVHD)预防包括移植后减少剂量的环磷酰胺(PTCy剂量减少50%)与霉酚酸酯和环孢素。他移植了完全的供体嵌合,第30天骨髓形态完全缓解,流式细胞术检测不到可测量的残留疾病。第126天,患者出现类固醇反应性晚发型II级急性GVHD (III期皮肤GVHD)。患者于第220天形态复发,第256天败血症合并感染性休克死亡。结论:该病例证明了单倍体- hct在DKC中使用基于曲硫丹的降低强度调节(RIC)方案和改良的基于ptc的GVHD预防的安全性和可行性。该患者的疾病复发强调了移植前疾病负担对不符合清髓条件的MDS/AML DKC患者无复发生存的影响。
Haploidentical Hematopoietic Cell Transplantation in Dyskeratosis Congenita with Myelodysplastic Syndrome/Acute Myeloid Leukemia.
Background: Allogeneic hematopoietic cell transplantation (Allo-HCT) is the only curative option for marrow failure, myelodysplastic syndrome (MDS), and acute myeloid leukemia associated with dyskeratosis congenita (DKC). Due to chromosomal instability and sensitivity to radiation and alkylating agents, HCT is associated with a high incidence of transplant-related mortality in DKC.
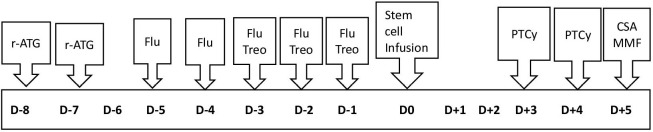
Case report: A 25-year-old male presented with DKC-associated cutaneous manifestations and myelodysplastic syndrome / acute myelogenous leukemia (MDS/AML). Targeted next-generation sequencing revealed mutation of the DKC1 and RUNX1 genes. His mother and sibling sisters were carriers for the DKC1 mutation. Due to high donor-specific antibody mean fluorescence intensity (DSA-MFI) against the unshared Human Leukocyte Antigen-A (HLA-A) allele of his 6/12 HLA-matched father, his paternal cousin's sister was selected as a haploidentical (6/12 HLA-matched) donor for HCT. He underwent allo-HCT with stable disease burden using a specifically-designed RIC regimen containing treosulfan (at 50% reduced dosing), fludarabine, and rabbit anti-thymocyte globulin. The graft versus host disease (GVHD) prophylaxis contained reduced-dose post-transplant cyclophosphamide (PTCy dose reduction of 50%) with mycophenolate mofetil and cyclosporine. He engrafted with complete donor chimerism, and the day +30 marrow was in complete morphological remission with undetectable measurable residual disease by flow cytometry. On day +126, he developed steroid-responsive late-onset grade II acute GVHD (stage III skin GVHD). He suffered from morphologic relapse on day +220 and succumbed from sepsis with septic shock on day +256.
Conclusion: This case demonstrates the safety and feasibility of haploidentical-HCT using a treosulfan-based reduced-intensity conditioning (RIC) regimen and modified PTCy-based GVHD prophylaxis in DKC. Disease relapse in this patient underscores the impact of pretransplant disease burden on relapse free survival in DKC patients with MDS/AML who are not eligible for myeloablative conditioning.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


