B F Pompeu, P Marcolin, F I L C B Marques, G A da Rocha Soares, A L C E Silva, B D'Andrea Pigossi, S M P de Figueiredo, F B Formiga
{"title":"扩展与有限肠系膜切除肠切除术治疗克罗恩病:荟萃分析和系统评价。","authors":"B F Pompeu, P Marcolin, F I L C B Marques, G A da Rocha Soares, A L C E Silva, B D'Andrea Pigossi, S M P de Figueiredo, F B Formiga","doi":"10.1007/s10151-024-03108-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is ongoing debate regarding the benefits of extended mesenteric excision (EME) versus limited mesenteric excision (LME) in intestinal resection for Crohn's disease (CD). Some studies suggest that EME may reduce surgical recurrence, which is defined as the need for reoperation due to disease complications or insufficient response to therapy, when compared with LME. This systematic review and meta-analysis aims to compare postoperative complications, surgical recurrence, and endoscopic recurrence in patients undergoing EME versus LME for CD.</p><p><strong>Methods: </strong>MEDLINE, Cochrane, the Central Register of Clinical Trials, Scopus and Web of Science databases were searched for studies published through April 2024. Odds ratios (OR) with 95% confidence intervals (CIs) were pooled using a random-effects model. Heterogeneity was assessed with Cochran's Q test and I<sup>2</sup> statistics, with p-values < 0.10 and I<sup>2</sup> > 25% considered significant. Statistical analyses were performed using R software, version 4.4.1.</p><p><strong>Results: </strong>One randomized controlled trial (RCT) and five observational studies were included, totaling 4498 patients, of whom 1059 (23.5%) underwent EME and 3439 (76.5%) LME. EME was associated with a lower surgical recurrence rate (5% versus 15%; OR 0.31; 95% CI 0.12-0.84; p = 0.021; I<sup>2</sup> = 47%). No significant differences were observed between EME and LME for overall complications, Clavien-Dindo ≥ 3 events, bleeding requiring transfusion, anastomotic leaks, intraabdominal abscesses, surgical site infections (SSIs), reoperations, readmissions, ileus, endoscopic recurrences, operative times, or hospital stays.</p><p><strong>Conclusions: </strong>EME was associated with a significant reduction in surgical recurrence compared with LME, without differences in endoscopic recurrence or postoperative complication rates.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"80"},"PeriodicalIF":2.9000,"publicationDate":"2025-03-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11891095/pdf/","citationCount":"0","resultStr":"{\"title\":\"Extended versus limited mesenteric excision in bowel resection for Crohn's disease: a meta-analysis and systematic review.\",\"authors\":\"B F Pompeu, P Marcolin, F I L C B Marques, G A da Rocha Soares, A L C E Silva, B D'Andrea Pigossi, S M P de Figueiredo, F B Formiga\",\"doi\":\"10.1007/s10151-024-03108-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is ongoing debate regarding the benefits of extended mesenteric excision (EME) versus limited mesenteric excision (LME) in intestinal resection for Crohn's disease (CD). Some studies suggest that EME may reduce surgical recurrence, which is defined as the need for reoperation due to disease complications or insufficient response to therapy, when compared with LME. This systematic review and meta-analysis aims to compare postoperative complications, surgical recurrence, and endoscopic recurrence in patients undergoing EME versus LME for CD.</p><p><strong>Methods: </strong>MEDLINE, Cochrane, the Central Register of Clinical Trials, Scopus and Web of Science databases were searched for studies published through April 2024. Odds ratios (OR) with 95% confidence intervals (CIs) were pooled using a random-effects model. Heterogeneity was assessed with Cochran's Q test and I<sup>2</sup> statistics, with p-values < 0.10 and I<sup>2</sup> > 25% considered significant. Statistical analyses were performed using R software, version 4.4.1.</p><p><strong>Results: </strong>One randomized controlled trial (RCT) and five observational studies were included, totaling 4498 patients, of whom 1059 (23.5%) underwent EME and 3439 (76.5%) LME. EME was associated with a lower surgical recurrence rate (5% versus 15%; OR 0.31; 95% CI 0.12-0.84; p = 0.021; I<sup>2</sup> = 47%). No significant differences were observed between EME and LME for overall complications, Clavien-Dindo ≥ 3 events, bleeding requiring transfusion, anastomotic leaks, intraabdominal abscesses, surgical site infections (SSIs), reoperations, readmissions, ileus, endoscopic recurrences, operative times, or hospital stays.</p><p><strong>Conclusions: </strong>EME was associated with a significant reduction in surgical recurrence compared with LME, without differences in endoscopic recurrence or postoperative complication rates.</p>\",\"PeriodicalId\":51192,\"journal\":{\"name\":\"Techniques in Coloproctology\",\"volume\":\"29 1\",\"pages\":\"80\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-03-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11891095/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Techniques in Coloproctology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10151-024-03108-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-024-03108-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
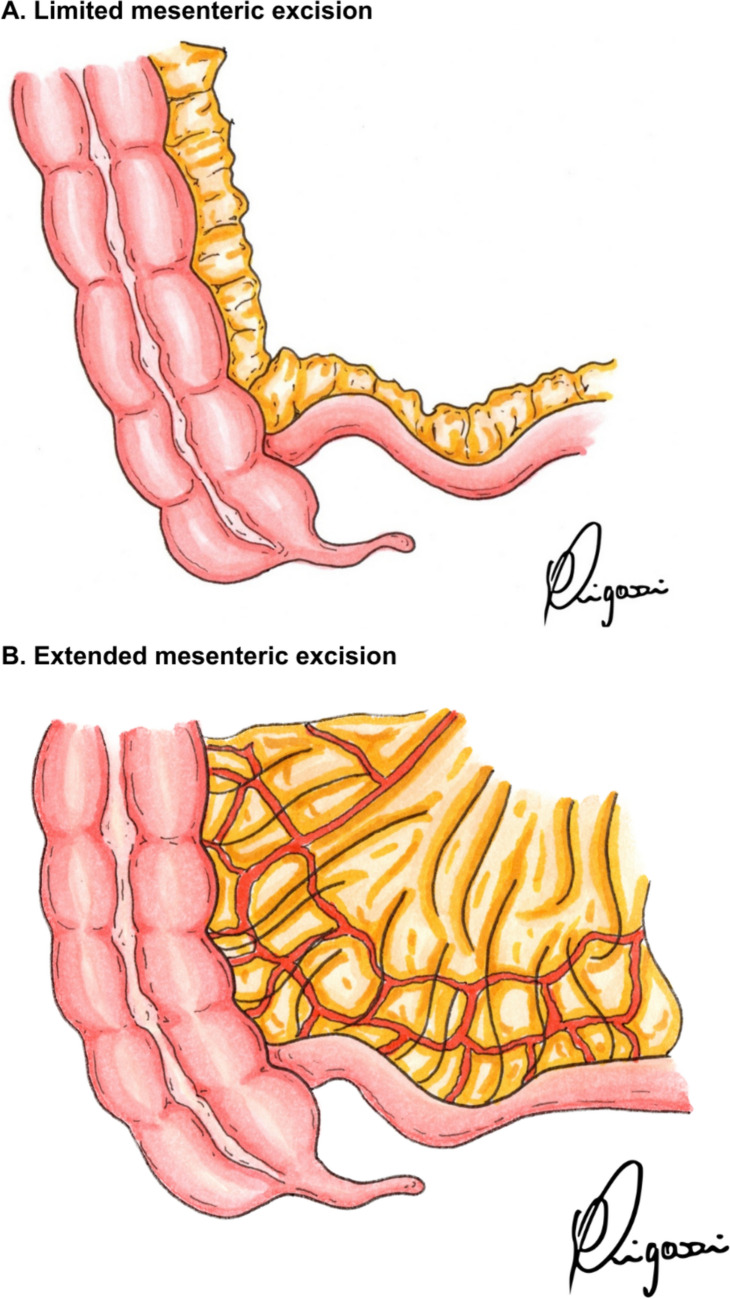
背景:在克罗恩病(CD)的肠切除术中,扩展肠系膜切除(EME)与有限肠系膜切除(LME)的益处一直存在争议。一些研究表明,与LME相比,EME可以减少手术复发,其定义是由于疾病并发症或对治疗反应不足而需要再次手术。本系统综述和荟萃分析旨在比较EME与LME患者的术后并发症、手术复发和内窥镜复发。方法:检索MEDLINE、Cochrane、中央临床试验注册、Scopus和Web of Science数据库,检索截至2024年4月发表的研究。比值比(OR)和95%置信区间(ci)采用随机效应模型进行汇总。异质性采用Cochran’s Q检验和I2统计量进行评估,p值为2 bb0 25%认为显著。采用R软件4.4.1进行统计分析。结果:纳入1项随机对照试验(RCT)和5项观察性研究,共4498例患者,其中1059例(23.5%)行EME, 3439例(76.5%)行LME。EME与较低的手术复发率相关(5%对15%;或0.31;95% ci 0.12-0.84;p = 0.021;i2 = 47%)。EME和LME在总并发症、Clavien-Dindo≥3事件、需要输血的出血、吻合口漏、腹内脓肿、手术部位感染(ssi)、再手术、再入院、肠梗阻、内镜下复发、手术时间或住院时间方面没有显著差异。结论:与LME相比,EME与手术复发率显著降低有关,在内镜下复发率和术后并发症发生率方面没有差异。
Extended versus limited mesenteric excision in bowel resection for Crohn's disease: a meta-analysis and systematic review.
Background: There is ongoing debate regarding the benefits of extended mesenteric excision (EME) versus limited mesenteric excision (LME) in intestinal resection for Crohn's disease (CD). Some studies suggest that EME may reduce surgical recurrence, which is defined as the need for reoperation due to disease complications or insufficient response to therapy, when compared with LME. This systematic review and meta-analysis aims to compare postoperative complications, surgical recurrence, and endoscopic recurrence in patients undergoing EME versus LME for CD.
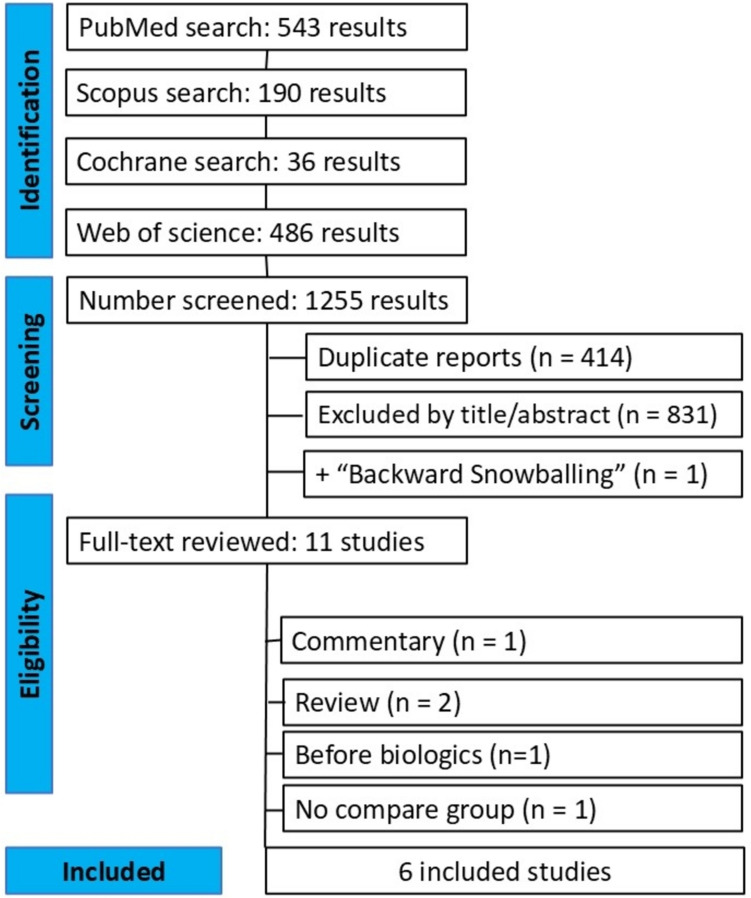
Methods: MEDLINE, Cochrane, the Central Register of Clinical Trials, Scopus and Web of Science databases were searched for studies published through April 2024. Odds ratios (OR) with 95% confidence intervals (CIs) were pooled using a random-effects model. Heterogeneity was assessed with Cochran's Q test and I2 statistics, with p-values < 0.10 and I2 > 25% considered significant. Statistical analyses were performed using R software, version 4.4.1.
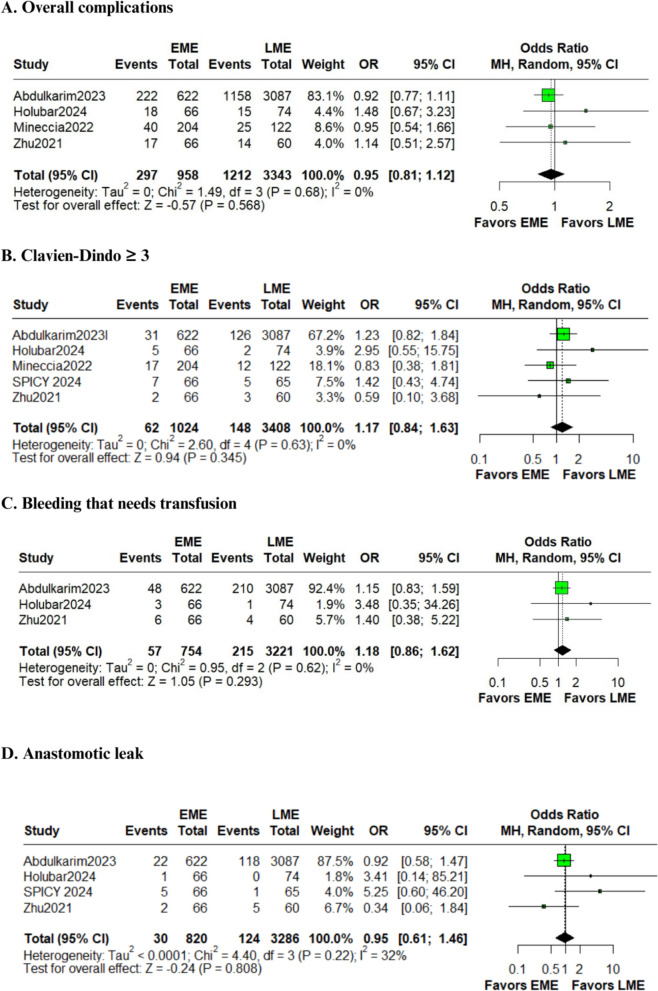
Results: One randomized controlled trial (RCT) and five observational studies were included, totaling 4498 patients, of whom 1059 (23.5%) underwent EME and 3439 (76.5%) LME. EME was associated with a lower surgical recurrence rate (5% versus 15%; OR 0.31; 95% CI 0.12-0.84; p = 0.021; I2 = 47%). No significant differences were observed between EME and LME for overall complications, Clavien-Dindo ≥ 3 events, bleeding requiring transfusion, anastomotic leaks, intraabdominal abscesses, surgical site infections (SSIs), reoperations, readmissions, ileus, endoscopic recurrences, operative times, or hospital stays.
Conclusions: EME was associated with a significant reduction in surgical recurrence compared with LME, without differences in endoscopic recurrence or postoperative complication rates.
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


