Mohammad Arabi, Hamdan S Alghamdi, Abdulaziz A Almesned, Omar I Alanazi, Khaled Alzahrani, Meshari A Alghamdi, Mohammed Bukhaytan, Mohammed F Alkhalaf, Muath A Almaimoni, Nawaf A Alagrafy, Farhan K Alanazi
{"title":"确定经动脉放射栓塞治疗的肝细胞癌患者死亡率和肝脏失代偿的关键预测因素。","authors":"Mohammad Arabi, Hamdan S Alghamdi, Abdulaziz A Almesned, Omar I Alanazi, Khaled Alzahrani, Meshari A Alghamdi, Mohammed Bukhaytan, Mohammed F Alkhalaf, Muath A Almaimoni, Nawaf A Alagrafy, Farhan K Alanazi","doi":"10.4103/sjg.sjg_343_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study aimed to identify the predictors of liver decompensation and mortality in patients with HCC treated with trans arterial radioembolization (TARE).</p><p><strong>Methods: </strong>A retrospective analysis of 140 HCC patients who underwent TARE was conducted. Kaplan-Meier and multivariate Cox regression analyses were performed to identify the key predictors of mortality and liver decompensation, defined as a total bilirubin level greater than 50 μmol/l or an upgrade in the Child-Pugh class within three months of the first TARE procedure.</p><p><strong>Results: </strong>The cohort comprised 69.3% males with a mean age of 71.3 ± 11.9 years. Most patients (73.6%) had Child-Pugh class A cirrhosis and 34.3% had BCLC stage B disease. Liver decompensation was recorded in 55 patients (39.2%) within three months of the first TARE procedure. A total of 80 patients (57.1%) died during the follow-up period. The median survival was significantly longer in those without liver decompensation (3.2 vs. 0.7 years, P < 0.001). Multivariate analysis revealed that male gender (adjusted odds ratio [aOR] 5.889, P = 0.009), cirrhosis (aOR 6.82, P = 0.047), and baseline international normalized ratio (INR) (aOR 316.664, P = 0.013) were independent predictors of liver decompensation. Cox regression analysis revealed several significant predictors of increased mortality including ascites (HR 2.012, 95% CI, 1.122-3.61; P = 0.019), portal vein invasion (HR 1.695, 95% CI, 1.057-2.718; P = 0.029), and diabetes mellitus (HR 1.823, 95% CI, 1.017-3.265; P = 0.044). Conversely, non-multifocal HCC (HR 0.593, 95% CI, 0.369-0.955; P = 0.031), treatment of the liver lobe other than the right lobe (HR, 0.482; 95% CI 0.236-0.986, P = 0.046), and age ≥60 years (HR 0.288, 95% CI, 0.139-0.597; P = 0.001) were associated with a reduced risk of mortality.</p><p><strong>Conclusion: </strong>This study identified the key predictors of liver decompensation and mortality in patients with HCC undergoing TARE, potentially improving patient selection and management strategies.</p>","PeriodicalId":48881,"journal":{"name":"Saudi Journal of Gastroenterology","volume":" ","pages":"176-184"},"PeriodicalIF":2.0000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12155456/pdf/","citationCount":"0","resultStr":"{\"title\":\"Identifying key predictors of mortality and liver decompensation in hepatocellular carcinoma patients treated with transarterial radioembolization.\",\"authors\":\"Mohammad Arabi, Hamdan S Alghamdi, Abdulaziz A Almesned, Omar I Alanazi, Khaled Alzahrani, Meshari A Alghamdi, Mohammed Bukhaytan, Mohammed F Alkhalaf, Muath A Almaimoni, Nawaf A Alagrafy, Farhan K Alanazi\",\"doi\":\"10.4103/sjg.sjg_343_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>This study aimed to identify the predictors of liver decompensation and mortality in patients with HCC treated with trans arterial radioembolization (TARE).</p><p><strong>Methods: </strong>A retrospective analysis of 140 HCC patients who underwent TARE was conducted. Kaplan-Meier and multivariate Cox regression analyses were performed to identify the key predictors of mortality and liver decompensation, defined as a total bilirubin level greater than 50 μmol/l or an upgrade in the Child-Pugh class within three months of the first TARE procedure.</p><p><strong>Results: </strong>The cohort comprised 69.3% males with a mean age of 71.3 ± 11.9 years. Most patients (73.6%) had Child-Pugh class A cirrhosis and 34.3% had BCLC stage B disease. Liver decompensation was recorded in 55 patients (39.2%) within three months of the first TARE procedure. A total of 80 patients (57.1%) died during the follow-up period. The median survival was significantly longer in those without liver decompensation (3.2 vs. 0.7 years, P < 0.001). Multivariate analysis revealed that male gender (adjusted odds ratio [aOR] 5.889, P = 0.009), cirrhosis (aOR 6.82, P = 0.047), and baseline international normalized ratio (INR) (aOR 316.664, P = 0.013) were independent predictors of liver decompensation. Cox regression analysis revealed several significant predictors of increased mortality including ascites (HR 2.012, 95% CI, 1.122-3.61; P = 0.019), portal vein invasion (HR 1.695, 95% CI, 1.057-2.718; P = 0.029), and diabetes mellitus (HR 1.823, 95% CI, 1.017-3.265; P = 0.044). Conversely, non-multifocal HCC (HR 0.593, 95% CI, 0.369-0.955; P = 0.031), treatment of the liver lobe other than the right lobe (HR, 0.482; 95% CI 0.236-0.986, P = 0.046), and age ≥60 years (HR 0.288, 95% CI, 0.139-0.597; P = 0.001) were associated with a reduced risk of mortality.</p><p><strong>Conclusion: </strong>This study identified the key predictors of liver decompensation and mortality in patients with HCC undergoing TARE, potentially improving patient selection and management strategies.</p>\",\"PeriodicalId\":48881,\"journal\":{\"name\":\"Saudi Journal of Gastroenterology\",\"volume\":\" \",\"pages\":\"176-184\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12155456/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Saudi Journal of Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4103/sjg.sjg_343_24\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/7 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Saudi Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4103/sjg.sjg_343_24","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/7 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:本研究旨在确定经动脉放射栓塞(TARE)治疗的HCC患者肝脏失代偿和死亡率的预测因素。方法:回顾性分析140例肝细胞癌患者行肝移植的临床资料。Kaplan-Meier和多变量Cox回归分析确定死亡率和肝脏失代偿的关键预测因素,定义为总胆红素水平大于50 μmol/l或在第一次TARE手术后三个月内Child-Pugh等级升级。结果:男性占69.3%,平均年龄71.3±11.9岁。大多数患者(73.6%)为Child-Pugh A级肝硬化,34.3%为BCLC B期疾病。55例患者(39.2%)在第一次TARE手术后3个月内出现肝脏失代偿。随访期间共死亡80例(57.1%)。无肝失代偿患者的中位生存期明显更长(3.2年vs. 0.7年,P < 0.001)。多因素分析显示,男性(校正优势比[aOR] 5.889, P = 0.009)、肝硬化(aOR 6.82, P = 0.047)和基线国际标准化比值(INR) (aOR 316.664, P = 0.013)是肝脏失代偿的独立预测因素。Cox回归分析显示了几个显著的死亡率增加的预测因素,包括腹水(HR 2.012, 95% CI, 1.122-3.61;P = 0.019),门静脉侵犯(HR 1.695, 95% CI 1.057 ~ 2.718;P = 0.029),糖尿病(HR 1.823, 95% CI, 1.017-3.265;P = 0.044)。相反,非多灶性HCC (HR 0.593, 95% CI, 0.369-0.955;P = 0.031),除右叶外肝叶治疗(HR, 0.482;95% CI 0.236 ~ 0.986, P = 0.046),年龄≥60岁(HR 0.288, 95% CI 0.139 ~ 0.597;P = 0.001)与死亡率降低相关。结论:本研究确定了肝细胞癌患者肝失代偿和死亡率的关键预测因素,可能改善患者选择和管理策略。
Identifying key predictors of mortality and liver decompensation in hepatocellular carcinoma patients treated with transarterial radioembolization.
Background: This study aimed to identify the predictors of liver decompensation and mortality in patients with HCC treated with trans arterial radioembolization (TARE).
Methods: A retrospective analysis of 140 HCC patients who underwent TARE was conducted. Kaplan-Meier and multivariate Cox regression analyses were performed to identify the key predictors of mortality and liver decompensation, defined as a total bilirubin level greater than 50 μmol/l or an upgrade in the Child-Pugh class within three months of the first TARE procedure.
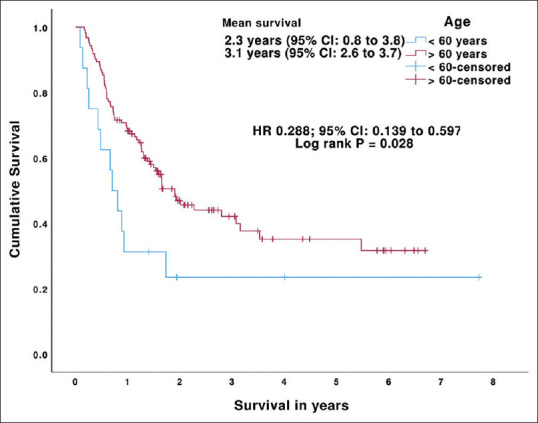
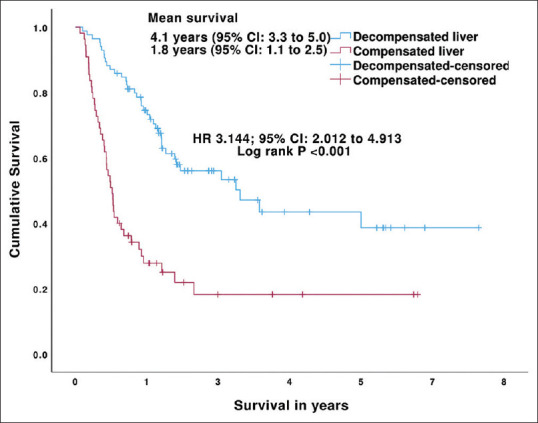
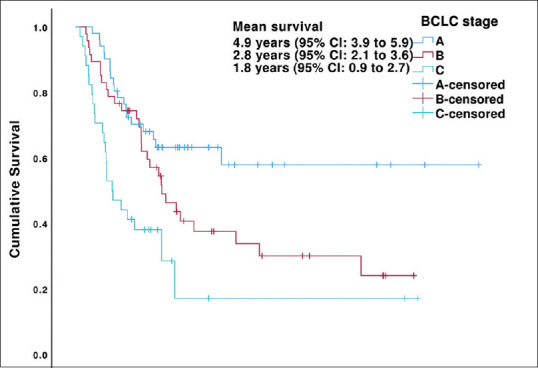
Results: The cohort comprised 69.3% males with a mean age of 71.3 ± 11.9 years. Most patients (73.6%) had Child-Pugh class A cirrhosis and 34.3% had BCLC stage B disease. Liver decompensation was recorded in 55 patients (39.2%) within three months of the first TARE procedure. A total of 80 patients (57.1%) died during the follow-up period. The median survival was significantly longer in those without liver decompensation (3.2 vs. 0.7 years, P < 0.001). Multivariate analysis revealed that male gender (adjusted odds ratio [aOR] 5.889, P = 0.009), cirrhosis (aOR 6.82, P = 0.047), and baseline international normalized ratio (INR) (aOR 316.664, P = 0.013) were independent predictors of liver decompensation. Cox regression analysis revealed several significant predictors of increased mortality including ascites (HR 2.012, 95% CI, 1.122-3.61; P = 0.019), portal vein invasion (HR 1.695, 95% CI, 1.057-2.718; P = 0.029), and diabetes mellitus (HR 1.823, 95% CI, 1.017-3.265; P = 0.044). Conversely, non-multifocal HCC (HR 0.593, 95% CI, 0.369-0.955; P = 0.031), treatment of the liver lobe other than the right lobe (HR, 0.482; 95% CI 0.236-0.986, P = 0.046), and age ≥60 years (HR 0.288, 95% CI, 0.139-0.597; P = 0.001) were associated with a reduced risk of mortality.
Conclusion: This study identified the key predictors of liver decompensation and mortality in patients with HCC undergoing TARE, potentially improving patient selection and management strategies.
期刊介绍:
The Saudi Journal of Gastroenterology (SJG) is an open access peer-reviewed publication. Authors are invited to submit articles in the field of gastroenterology, hepatology and nutrition, with a wide spectrum of coverage including basic science, epidemiology, diagnostics, therapeutics, public health, and standards of health care in relation to the concerned specialty. Review articles are usually by invitation. However review articles of current interest and a high standard of scientific value could also be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


