Patrick Goodley, Haval Balata, Hilary A Robbins, Richard Booton, Matthew Sperrin, Philip A J Crosbie
{"title":"曼彻斯特肺部健康检查队列中肺癌筛查基于风险选择的6年表现","authors":"Patrick Goodley, Haval Balata, Hilary A Robbins, Richard Booton, Matthew Sperrin, Philip A J Crosbie","doi":"10.1136/bmjonc-2024-000560","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Risk prediction models are used to determine eligibility for targeted lung cancer screening. However, prospective data regarding model performance in this setting are limited. Here we report the performance of the PLCO<sub>m2012</sub> risk model, which calculates 6 year lung cancer risk, in a cohort invited for lung cancer screening in a socioeconomically deprived area.</p><p><strong>Methods and analysis: </strong>Calibration (expected/observed (E/O) lung cancer diagnoses over 6 years) and discrimination (area under the receiver operating characteristic curve) of PLCO<sub>m2012</sub> and other models was performed in Manchester Lung Health Check (M-LHC) participants, where PLCO<sub>m2012</sub> ≥1.51% was used prospectively to determine screening eligibility. Lung cancers diagnosed by any route were captured within 6 years of risk assessment, for both screened and non-screened participants. Performance of a range of models was evaluated.</p><p><strong>Results: </strong>Out of 2541 attendees, 56% were high-risk (n=1430/2541) and offered screening; 44% were low-risk (n=1111/2541) and not screened. Over 6 years, 7.3% (n=105/1430) and 0.9% (n=10/1111) were diagnosed with lung cancer in the high and low-risk cohorts, respectively (p<0.0001). Risk was underestimated in both high-risk, screened (E/O 0.68 (0.57-0.82)) and low-risk, unscreened groups (E/O 0.61 (0.33-1.14)). Most other models also underestimated risk.</p><p><strong>Conclusion: </strong>Risk-based eligibility using PLCO<sub>m2012</sub> successfully classified most eventual lung cancer cases in the high-risk, screened group. Prediction models generally underestimated risk in this socioeconomically deprived cohort, irrespective of screening status. The effect of screening on increasing the probability of lung cancer diagnosis should be considered when interpreting measures of prediction model performance.</p>","PeriodicalId":72436,"journal":{"name":"BMJ oncology","volume":"3 1","pages":"e000560"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880782/pdf/","citationCount":"0","resultStr":"{\"title\":\"Six-year performance of risk-based selection for lung cancer screening in the Manchester Lung Health Check cohort.\",\"authors\":\"Patrick Goodley, Haval Balata, Hilary A Robbins, Richard Booton, Matthew Sperrin, Philip A J Crosbie\",\"doi\":\"10.1136/bmjonc-2024-000560\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Risk prediction models are used to determine eligibility for targeted lung cancer screening. However, prospective data regarding model performance in this setting are limited. Here we report the performance of the PLCO<sub>m2012</sub> risk model, which calculates 6 year lung cancer risk, in a cohort invited for lung cancer screening in a socioeconomically deprived area.</p><p><strong>Methods and analysis: </strong>Calibration (expected/observed (E/O) lung cancer diagnoses over 6 years) and discrimination (area under the receiver operating characteristic curve) of PLCO<sub>m2012</sub> and other models was performed in Manchester Lung Health Check (M-LHC) participants, where PLCO<sub>m2012</sub> ≥1.51% was used prospectively to determine screening eligibility. Lung cancers diagnosed by any route were captured within 6 years of risk assessment, for both screened and non-screened participants. Performance of a range of models was evaluated.</p><p><strong>Results: </strong>Out of 2541 attendees, 56% were high-risk (n=1430/2541) and offered screening; 44% were low-risk (n=1111/2541) and not screened. Over 6 years, 7.3% (n=105/1430) and 0.9% (n=10/1111) were diagnosed with lung cancer in the high and low-risk cohorts, respectively (p<0.0001). Risk was underestimated in both high-risk, screened (E/O 0.68 (0.57-0.82)) and low-risk, unscreened groups (E/O 0.61 (0.33-1.14)). Most other models also underestimated risk.</p><p><strong>Conclusion: </strong>Risk-based eligibility using PLCO<sub>m2012</sub> successfully classified most eventual lung cancer cases in the high-risk, screened group. Prediction models generally underestimated risk in this socioeconomically deprived cohort, irrespective of screening status. The effect of screening on increasing the probability of lung cancer diagnosis should be considered when interpreting measures of prediction model performance.</p>\",\"PeriodicalId\":72436,\"journal\":{\"name\":\"BMJ oncology\",\"volume\":\"3 1\",\"pages\":\"e000560\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11880782/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjonc-2024-000560\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjonc-2024-000560","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Six-year performance of risk-based selection for lung cancer screening in the Manchester Lung Health Check cohort.
Objective: Risk prediction models are used to determine eligibility for targeted lung cancer screening. However, prospective data regarding model performance in this setting are limited. Here we report the performance of the PLCOm2012 risk model, which calculates 6 year lung cancer risk, in a cohort invited for lung cancer screening in a socioeconomically deprived area.
Methods and analysis: Calibration (expected/observed (E/O) lung cancer diagnoses over 6 years) and discrimination (area under the receiver operating characteristic curve) of PLCOm2012 and other models was performed in Manchester Lung Health Check (M-LHC) participants, where PLCOm2012 ≥1.51% was used prospectively to determine screening eligibility. Lung cancers diagnosed by any route were captured within 6 years of risk assessment, for both screened and non-screened participants. Performance of a range of models was evaluated.
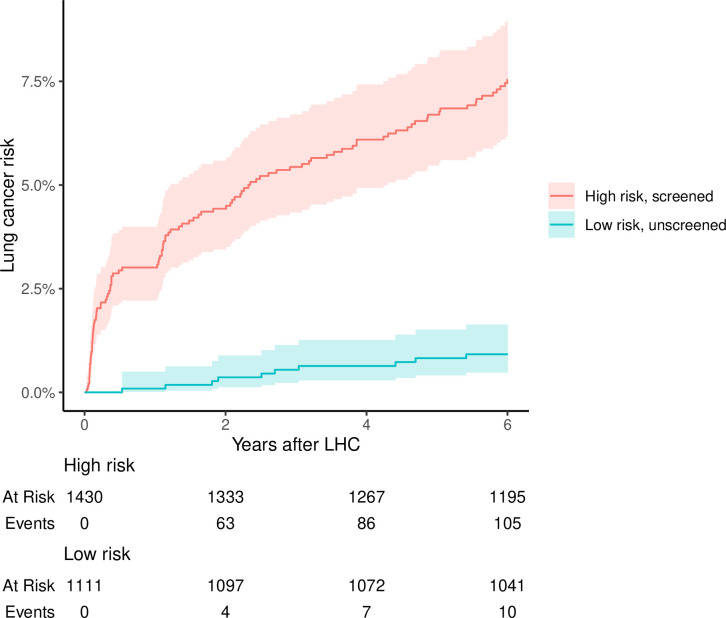
Results: Out of 2541 attendees, 56% were high-risk (n=1430/2541) and offered screening; 44% were low-risk (n=1111/2541) and not screened. Over 6 years, 7.3% (n=105/1430) and 0.9% (n=10/1111) were diagnosed with lung cancer in the high and low-risk cohorts, respectively (p<0.0001). Risk was underestimated in both high-risk, screened (E/O 0.68 (0.57-0.82)) and low-risk, unscreened groups (E/O 0.61 (0.33-1.14)). Most other models also underestimated risk.
Conclusion: Risk-based eligibility using PLCOm2012 successfully classified most eventual lung cancer cases in the high-risk, screened group. Prediction models generally underestimated risk in this socioeconomically deprived cohort, irrespective of screening status. The effect of screening on increasing the probability of lung cancer diagnosis should be considered when interpreting measures of prediction model performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


