Katy A Chalmers, Matthew J Lee, Sian E Cousins, Adam Peckham Cooper, Peter O Coe, Natalie S Blencowe
{"title":"腹腔镜与开放式修复穿孔性消化性溃疡:系统的范围审查和现有证据的深入评估。","authors":"Katy A Chalmers, Matthew J Lee, Sian E Cousins, Adam Peckham Cooper, Peter O Coe, Natalie S Blencowe","doi":"10.1093/bjsopen/zrae163","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Perforated peptic ulcer remains a common contributor to morbidity and mortality rates worldwide. In common with other emergency surgery conditions, there is a trend towards minimally invasive surgery. This review aims to describe current evidence comparing open and laparoscopic management strategies for perforated peptic ulcers, by summarizing patients, intervention, comparator, outcomes, describing intervention components and delivery, outcomes reported and assessing study pragmatism (applicability) using PRagmatic Explanatory Continuum Indicator Summary-2.</p><p><strong>Methods: </strong>Systematic searches of published literature were performed using Ovid MEDLINE and Embase online databases, as well as clinical trial databases. Randomized trials comparing laparoscopic and open repair of peptic ulcer were included. Data extracted included study metadata, patients, intervention, comparator, outcomes elements, technical aspects of interventions and use of co-interventions, and surgeon learning curves/experience. Applicability was assessed using the PRagmatic Explanatory Continuum Indicator Summary-2 tool, to explore whether trials were predominantly pragmatic or explanatory, and study validity assessed using the Cochrane Risk-of-Bias 2 tool.</p><p><strong>Results: </strong>A total of 408 studies were screened for eligibility, with nine finally included (880 patients). Incision, ulcer closure details and lavage were the most frequently reported aspects of laparoscopic repair. Co-interventions such as antibiotic use and analgesia were reported in most articles, whilst nutrition and Helicobacter pylori eradication were not reported. Interventions were generally delivered by high-volume laparoscopic surgeons. Studies were considered at high Risk-of-Bias. PRagmatic Explanatory Continuum Indicator Summary-2 assessment found studies were neither fully pragmatic nor explanatory.</p><p><strong>Conclusion: </strong>Laparoscopic repair of perforated peptic ulcer is a variably defined intervention. Consideration of how intervention components and co-interventions should be optimally delivered is required to facilitate a well designed randomized trial.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"9 2","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11882505/pdf/","citationCount":"0","resultStr":"{\"title\":\"Laparoscopic versus open repair of perforated peptic ulcer: systematic scoping review and in-depth evaluation of existing evidence.\",\"authors\":\"Katy A Chalmers, Matthew J Lee, Sian E Cousins, Adam Peckham Cooper, Peter O Coe, Natalie S Blencowe\",\"doi\":\"10.1093/bjsopen/zrae163\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Perforated peptic ulcer remains a common contributor to morbidity and mortality rates worldwide. In common with other emergency surgery conditions, there is a trend towards minimally invasive surgery. This review aims to describe current evidence comparing open and laparoscopic management strategies for perforated peptic ulcers, by summarizing patients, intervention, comparator, outcomes, describing intervention components and delivery, outcomes reported and assessing study pragmatism (applicability) using PRagmatic Explanatory Continuum Indicator Summary-2.</p><p><strong>Methods: </strong>Systematic searches of published literature were performed using Ovid MEDLINE and Embase online databases, as well as clinical trial databases. Randomized trials comparing laparoscopic and open repair of peptic ulcer were included. Data extracted included study metadata, patients, intervention, comparator, outcomes elements, technical aspects of interventions and use of co-interventions, and surgeon learning curves/experience. Applicability was assessed using the PRagmatic Explanatory Continuum Indicator Summary-2 tool, to explore whether trials were predominantly pragmatic or explanatory, and study validity assessed using the Cochrane Risk-of-Bias 2 tool.</p><p><strong>Results: </strong>A total of 408 studies were screened for eligibility, with nine finally included (880 patients). Incision, ulcer closure details and lavage were the most frequently reported aspects of laparoscopic repair. Co-interventions such as antibiotic use and analgesia were reported in most articles, whilst nutrition and Helicobacter pylori eradication were not reported. Interventions were generally delivered by high-volume laparoscopic surgeons. Studies were considered at high Risk-of-Bias. PRagmatic Explanatory Continuum Indicator Summary-2 assessment found studies were neither fully pragmatic nor explanatory.</p><p><strong>Conclusion: </strong>Laparoscopic repair of perforated peptic ulcer is a variably defined intervention. Consideration of how intervention components and co-interventions should be optimally delivered is required to facilitate a well designed randomized trial.</p>\",\"PeriodicalId\":9028,\"journal\":{\"name\":\"BJS Open\",\"volume\":\"9 2\",\"pages\":\"\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2025-03-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11882505/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BJS Open\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/bjsopen/zrae163\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae163","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
Laparoscopic versus open repair of perforated peptic ulcer: systematic scoping review and in-depth evaluation of existing evidence.
Background: Perforated peptic ulcer remains a common contributor to morbidity and mortality rates worldwide. In common with other emergency surgery conditions, there is a trend towards minimally invasive surgery. This review aims to describe current evidence comparing open and laparoscopic management strategies for perforated peptic ulcers, by summarizing patients, intervention, comparator, outcomes, describing intervention components and delivery, outcomes reported and assessing study pragmatism (applicability) using PRagmatic Explanatory Continuum Indicator Summary-2.
Methods: Systematic searches of published literature were performed using Ovid MEDLINE and Embase online databases, as well as clinical trial databases. Randomized trials comparing laparoscopic and open repair of peptic ulcer were included. Data extracted included study metadata, patients, intervention, comparator, outcomes elements, technical aspects of interventions and use of co-interventions, and surgeon learning curves/experience. Applicability was assessed using the PRagmatic Explanatory Continuum Indicator Summary-2 tool, to explore whether trials were predominantly pragmatic or explanatory, and study validity assessed using the Cochrane Risk-of-Bias 2 tool.
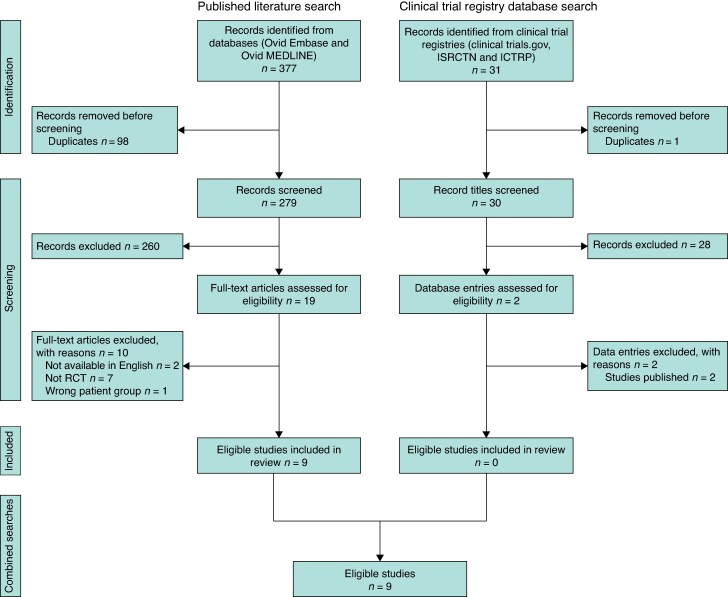
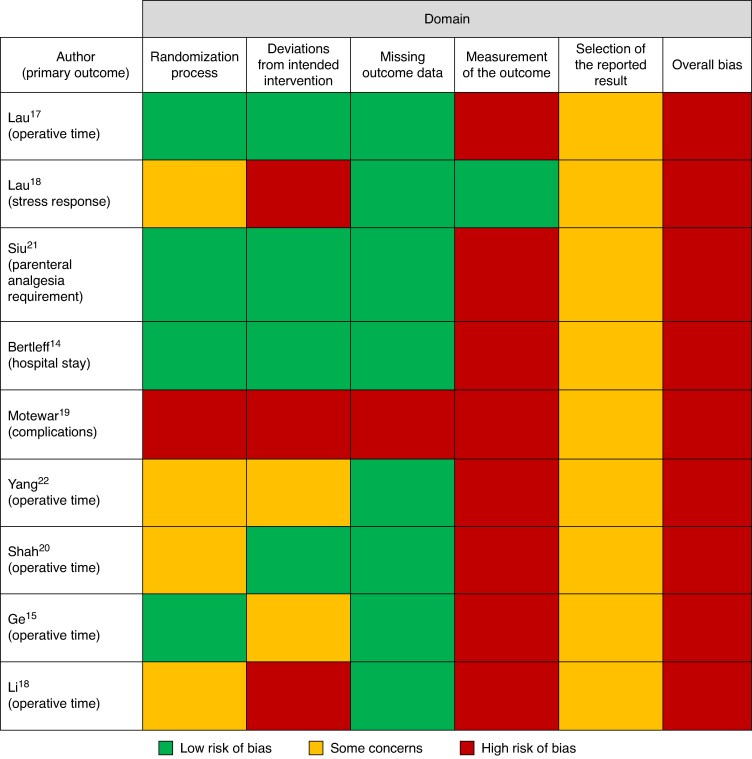
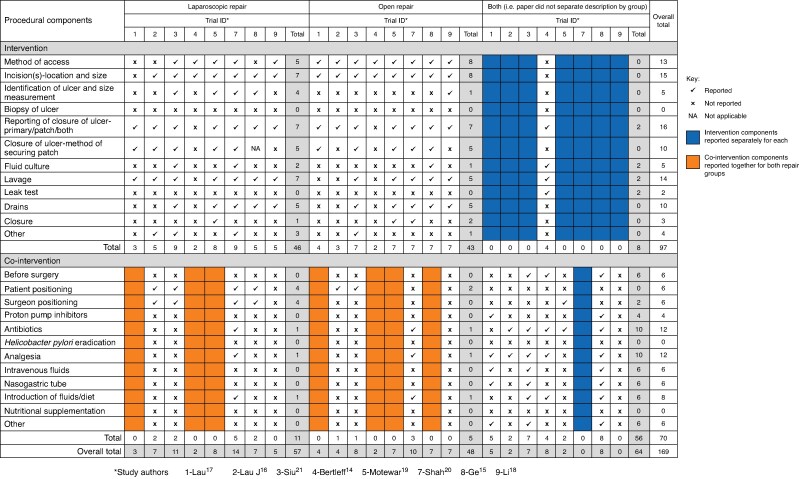
Results: A total of 408 studies were screened for eligibility, with nine finally included (880 patients). Incision, ulcer closure details and lavage were the most frequently reported aspects of laparoscopic repair. Co-interventions such as antibiotic use and analgesia were reported in most articles, whilst nutrition and Helicobacter pylori eradication were not reported. Interventions were generally delivered by high-volume laparoscopic surgeons. Studies were considered at high Risk-of-Bias. PRagmatic Explanatory Continuum Indicator Summary-2 assessment found studies were neither fully pragmatic nor explanatory.
Conclusion: Laparoscopic repair of perforated peptic ulcer is a variably defined intervention. Consideration of how intervention components and co-interventions should be optimally delivered is required to facilitate a well designed randomized trial.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


