Bryony Beal, Luke Buizen, Emily K Yeung, Lauren Heath, Lauren Houston, David Z I Cherney, Meg Jardine, Carol Pollock, Clare Arnott, Sradha S Kotwal, Hiddo J L Heerspink, Vlado Perkovic, Brendon L Neuen
{"title":"SGLT2抑制对CKD和2型糖尿病患者胰岛素使用的影响:CREDENCE试验的见解","authors":"Bryony Beal, Luke Buizen, Emily K Yeung, Lauren Heath, Lauren Houston, David Z I Cherney, Meg Jardine, Carol Pollock, Clare Arnott, Sradha S Kotwal, Hiddo J L Heerspink, Vlado Perkovic, Brendon L Neuen","doi":"10.1093/ndt/gfaf044","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Insulin is a mainstay treatment for diabetes, but its use is associated with weight gain and hypoglycaemia. Data on the effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on insulin use in people with chronic kidney disease (CKD) are limited.</p><p><strong>Methods: </strong>We conducted a post hoc analysis of the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation trial. Effects of canagliflozin versus placebo on insulin use (initiation, dose intensification, reduction and discontinuation) in people with CKD and type 2 diabetes were evaluated using Cox regression models. The primary outcome was insulin initiation or a >25% insulin dose intensification (in those not receiving and receiving insulin at baseline, respectively). Effects on kidney, cardiovascular and safety outcomes by baseline insulin use were also assessed.</p><p><strong>Results: </strong>Among 4401 participants, 2884 (65.5%) were receiving insulin at baseline; these participants were more likely to have lower estimated glomerular filtration rate, higher albuminuria and a longer duration of diabetes (all P < .001). Over a median on-treatment period of 2.0 years, canagliflozin reduced the need for insulin initiation or a >25% dose intensification by 19% compared with placebo {hazard ratio [HR] 0.81 [95% confidence interval (CI) 0.71-0.93]}, irrespective of baseline kidney function or albuminuria (both P-interaction > .10). Sustained insulin dose reductions of >50% were achieved more frequently with canagliflozin than placebo [HR 1.49 (95% CI 1.15-1.91)], although no difference in insulin discontinuation was observed between treatment arms. Effects of canagliflozin on kidney, cardiovascular and safety outcomes were consistent regardless of baseline insulin use (all P-interaction > .05).</p><p><strong>Conclusions: </strong>In CKD and type 2 diabetes, canagliflozin reduces insulin use with consistent effects regardless of baseline kidney function. This supports the use of canagliflozin in people with CKD, not only for end-organ protection, but also to improve glycaemic control and reduce exposure to insulin and its associated adverse effects.</p>","PeriodicalId":19078,"journal":{"name":"Nephrology Dialysis Transplantation","volume":" ","pages":"1727-1735"},"PeriodicalIF":5.6000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394126/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effects of SGLT2 inhibition on insulin use in CKD and type 2 diabetes: insights from the CREDENCE trial.\",\"authors\":\"Bryony Beal, Luke Buizen, Emily K Yeung, Lauren Heath, Lauren Houston, David Z I Cherney, Meg Jardine, Carol Pollock, Clare Arnott, Sradha S Kotwal, Hiddo J L Heerspink, Vlado Perkovic, Brendon L Neuen\",\"doi\":\"10.1093/ndt/gfaf044\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Insulin is a mainstay treatment for diabetes, but its use is associated with weight gain and hypoglycaemia. Data on the effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on insulin use in people with chronic kidney disease (CKD) are limited.</p><p><strong>Methods: </strong>We conducted a post hoc analysis of the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation trial. Effects of canagliflozin versus placebo on insulin use (initiation, dose intensification, reduction and discontinuation) in people with CKD and type 2 diabetes were evaluated using Cox regression models. The primary outcome was insulin initiation or a >25% insulin dose intensification (in those not receiving and receiving insulin at baseline, respectively). Effects on kidney, cardiovascular and safety outcomes by baseline insulin use were also assessed.</p><p><strong>Results: </strong>Among 4401 participants, 2884 (65.5%) were receiving insulin at baseline; these participants were more likely to have lower estimated glomerular filtration rate, higher albuminuria and a longer duration of diabetes (all P < .001). Over a median on-treatment period of 2.0 years, canagliflozin reduced the need for insulin initiation or a >25% dose intensification by 19% compared with placebo {hazard ratio [HR] 0.81 [95% confidence interval (CI) 0.71-0.93]}, irrespective of baseline kidney function or albuminuria (both P-interaction > .10). Sustained insulin dose reductions of >50% were achieved more frequently with canagliflozin than placebo [HR 1.49 (95% CI 1.15-1.91)], although no difference in insulin discontinuation was observed between treatment arms. Effects of canagliflozin on kidney, cardiovascular and safety outcomes were consistent regardless of baseline insulin use (all P-interaction > .05).</p><p><strong>Conclusions: </strong>In CKD and type 2 diabetes, canagliflozin reduces insulin use with consistent effects regardless of baseline kidney function. This supports the use of canagliflozin in people with CKD, not only for end-organ protection, but also to improve glycaemic control and reduce exposure to insulin and its associated adverse effects.</p>\",\"PeriodicalId\":19078,\"journal\":{\"name\":\"Nephrology Dialysis Transplantation\",\"volume\":\" \",\"pages\":\"1727-1735\"},\"PeriodicalIF\":5.6000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394126/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephrology Dialysis Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ndt/gfaf044\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephrology Dialysis Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ndt/gfaf044","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
摘要
背景:胰岛素是糖尿病的主要治疗方法,但它的使用与体重增加和低血糖有关。关于钠-葡萄糖共转运蛋白2 (SGLT2)抑制剂对慢性肾脏疾病(CKD)患者胰岛素使用的影响的数据有限。方法:我们对CREDENCE (canag列净与糖尿病肾病患者肾脏事件的临床评价)试验进行了事后分析。使用Cox回归模型评估了卡格列净与安慰剂对CKD和2型糖尿病患者胰岛素使用(起始、剂量强化、减少和停药)的影响。主要结局是胰岛素起始或bbb25 %胰岛素剂量强化(分别在基线时未接受胰岛素治疗和接受胰岛素治疗的患者中)。基线胰岛素使用对肾脏、心血管和安全性的影响也进行了评估。结果:在4401名参与者中,2884名(65.5%)在基线时接受胰岛素治疗;这些参与者更有可能有较低的估计肾小球滤过率,较高的蛋白尿和较长的糖尿病持续时间(与安慰剂相比,所有P25%剂量增强19% (HR 0.81, 95% CI 0.71-0.93),无论基线肾功能或蛋白尿(p -相互作用>0.10)。卡格列净组比安慰剂组更频繁地实现胰岛素剂量持续减少50 - 50% (HR 1.49, 95% CI 1.15-1.91),尽管在治疗组之间没有观察到胰岛素停用的差异。不管基线胰岛素使用情况如何,卡格列净对肾脏、心血管和安全性的影响是一致的(所有p相互作用>.05)。结论:在CKD和2型糖尿病患者中,无论基线肾功能如何,卡格列净都能减少胰岛素的使用。这支持在CKD患者中使用canagliflozin,不仅可以保护终末器官,还可以改善血糖控制,减少胰岛素暴露及其相关不良反应。
Effects of SGLT2 inhibition on insulin use in CKD and type 2 diabetes: insights from the CREDENCE trial.
Background: Insulin is a mainstay treatment for diabetes, but its use is associated with weight gain and hypoglycaemia. Data on the effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on insulin use in people with chronic kidney disease (CKD) are limited.
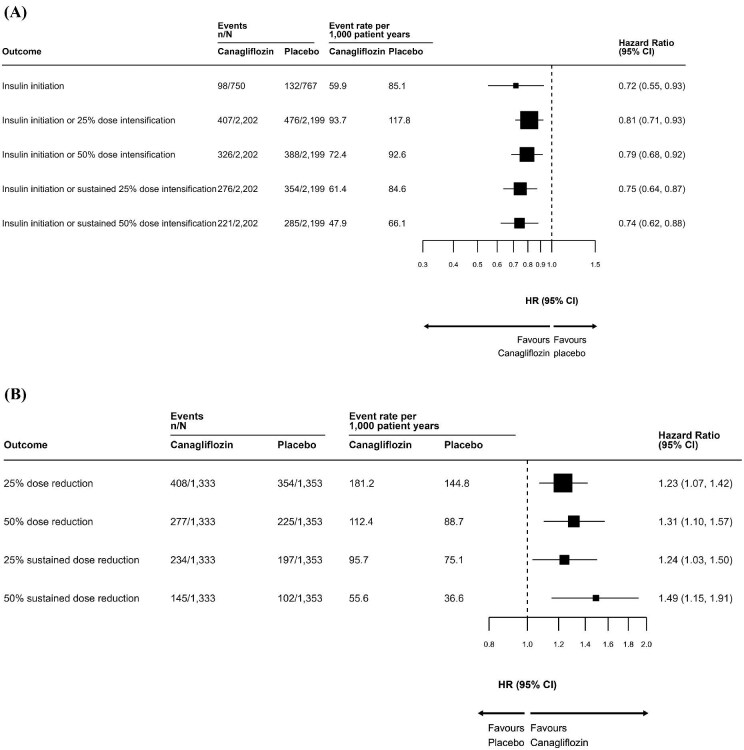
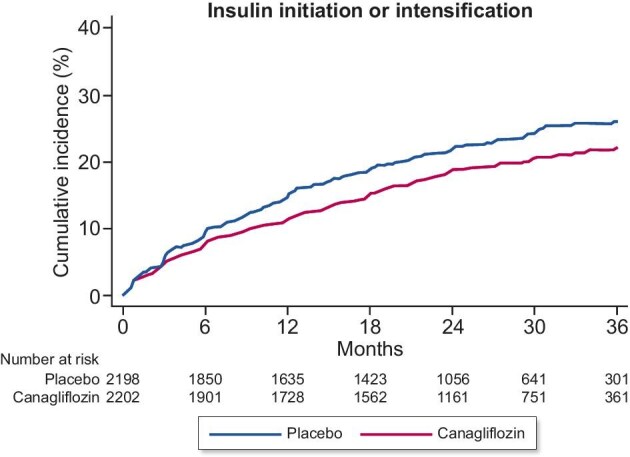
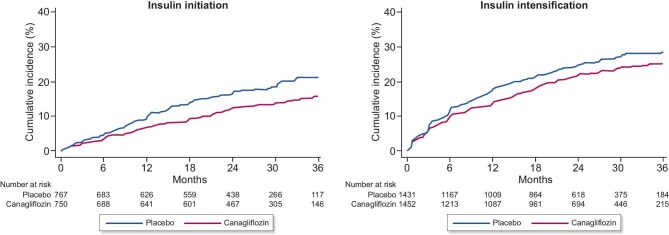
Methods: We conducted a post hoc analysis of the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation trial. Effects of canagliflozin versus placebo on insulin use (initiation, dose intensification, reduction and discontinuation) in people with CKD and type 2 diabetes were evaluated using Cox regression models. The primary outcome was insulin initiation or a >25% insulin dose intensification (in those not receiving and receiving insulin at baseline, respectively). Effects on kidney, cardiovascular and safety outcomes by baseline insulin use were also assessed.
Results: Among 4401 participants, 2884 (65.5%) were receiving insulin at baseline; these participants were more likely to have lower estimated glomerular filtration rate, higher albuminuria and a longer duration of diabetes (all P < .001). Over a median on-treatment period of 2.0 years, canagliflozin reduced the need for insulin initiation or a >25% dose intensification by 19% compared with placebo {hazard ratio [HR] 0.81 [95% confidence interval (CI) 0.71-0.93]}, irrespective of baseline kidney function or albuminuria (both P-interaction > .10). Sustained insulin dose reductions of >50% were achieved more frequently with canagliflozin than placebo [HR 1.49 (95% CI 1.15-1.91)], although no difference in insulin discontinuation was observed between treatment arms. Effects of canagliflozin on kidney, cardiovascular and safety outcomes were consistent regardless of baseline insulin use (all P-interaction > .05).
Conclusions: In CKD and type 2 diabetes, canagliflozin reduces insulin use with consistent effects regardless of baseline kidney function. This supports the use of canagliflozin in people with CKD, not only for end-organ protection, but also to improve glycaemic control and reduce exposure to insulin and its associated adverse effects.
期刊介绍:
Nephrology Dialysis Transplantation (ndt) is the leading nephrology journal in Europe and renowned worldwide, devoted to original clinical and laboratory research in nephrology, dialysis and transplantation. ndt is an official journal of the [ERA-EDTA](http://www.era-edta.org/) (European Renal Association-European Dialysis and Transplant Association). Published monthly, the journal provides an essential resource for researchers and clinicians throughout the world. All research articles in this journal have undergone peer review.
Print ISSN: 0931-0509.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


