Mirthe H W Van Veghel, Liza N Van Steenbergen, Cornelis P J Visser, B Willem Schreurs, Gerjon Hannink
{"title":"确定初次全肩关节置换术后的恢复轨迹:一项来自荷兰关节置换术登记的3358例患者的队列研究。","authors":"Mirthe H W Van Veghel, Liza N Van Steenbergen, Cornelis P J Visser, B Willem Schreurs, Gerjon Hannink","doi":"10.2340/17453674.2025.43085","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Some patients do not improve after total shoulder arthroplasty (TSA), indicating different recovery trajectories. We aimed to identify recovery trajectories after TSA based on the Oxford Shoulder Score (OSS). Second, we investigated whether recovery trajectories were associated with patient or procedure characteristics.</p><p><strong>Methods: </strong>We included primary anatomical and reversed TSAs (ATSAs/RTSAs) for osteoarthritis (OA) or cuff arthropathy/rupture with preoperative, 3-month, and/or 12-month postoperative OSS, registered between 2016 and 2022 in the Dutch Arthroplasty Register (n = 3,358). We used latent class growth modeling (LCGM) to identify recovery patterns, and multinomial logistic regression analyses to investigate associations between potential risk factors and class membership (odds ratio [OR], 95% confidence interval [CI]).</p><p><strong>Results: </strong>We identified 3 recovery patterns: \"Fast responders\" (59%), \"Steady responders\" (27%), and \"Poor responders\" (14%). Factors associated with \"Steady responders\" vs \"Fast responders\" were female vs male sex (OR 2.0, CI 1.5-2.7), ASA III-IV vs ASA I (OR 1.9, CI 1.2-3.1), Walch A1 vs B2 (OR 1.6, CI 1.1-2.5), and most vs medium socioeconomic deprivation (OR 1.4, CI 1.1-1.9). Factors associated with \"Poor responders\" vs \"Fast responders\" were ASA II vs ASA I (OR 2.0, CI 1.1-3.6), ASA III-IV vs ASA I (OR 3.0, CI 1.6-5.5), Walch A1 vs B2 (OR 2.1, CI 1.3-3.3), previous shoulder surgeries (OR 1.8, CI 1.3-2.4), most vs medium socioeconomic deprivation (OR 1.5, CI 1.2-2.0), RTSA for OA vs ATSA for OA (OR 1.8, CI 1.2-2.7), and RTSA for cuff arthropathy or rupture vs ATSA for OA (OR 2.3, CI 1.5-3.4).</p><p><strong>Conclusion: </strong>3 recovery trajectories were identified following TSA, which we labelled as \"Fast responders,\" \"Steady responders,\" and \"Poor responders.\" \"Steady responders\" and \"Poor responders\" were more likely to have higher ASA scores, a Walch A1 vs B2 classification, and greater vs medium socioeconomic deprivation than \"Fast responders.\" Moreover, \"Steady responders\" were more likely to be female, while \"Poor responders\" were more likely to have previous shoulder surgeries and RTSA for OA or for cuff arthropathy or rupture than \"Fast responders.\"</p>","PeriodicalId":6916,"journal":{"name":"Acta Orthopaedica","volume":"96 ","pages":"226-234"},"PeriodicalIF":2.4000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11881023/pdf/","citationCount":"0","resultStr":"{\"title\":\"Identifying recovery trajectories following primary total shoulder arthroplasty: a cohort study of 3,358 patients from the Dutch Arthroplasty Register.\",\"authors\":\"Mirthe H W Van Veghel, Liza N Van Steenbergen, Cornelis P J Visser, B Willem Schreurs, Gerjon Hannink\",\"doi\":\"10.2340/17453674.2025.43085\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Some patients do not improve after total shoulder arthroplasty (TSA), indicating different recovery trajectories. We aimed to identify recovery trajectories after TSA based on the Oxford Shoulder Score (OSS). Second, we investigated whether recovery trajectories were associated with patient or procedure characteristics.</p><p><strong>Methods: </strong>We included primary anatomical and reversed TSAs (ATSAs/RTSAs) for osteoarthritis (OA) or cuff arthropathy/rupture with preoperative, 3-month, and/or 12-month postoperative OSS, registered between 2016 and 2022 in the Dutch Arthroplasty Register (n = 3,358). We used latent class growth modeling (LCGM) to identify recovery patterns, and multinomial logistic regression analyses to investigate associations between potential risk factors and class membership (odds ratio [OR], 95% confidence interval [CI]).</p><p><strong>Results: </strong>We identified 3 recovery patterns: \\\"Fast responders\\\" (59%), \\\"Steady responders\\\" (27%), and \\\"Poor responders\\\" (14%). Factors associated with \\\"Steady responders\\\" vs \\\"Fast responders\\\" were female vs male sex (OR 2.0, CI 1.5-2.7), ASA III-IV vs ASA I (OR 1.9, CI 1.2-3.1), Walch A1 vs B2 (OR 1.6, CI 1.1-2.5), and most vs medium socioeconomic deprivation (OR 1.4, CI 1.1-1.9). Factors associated with \\\"Poor responders\\\" vs \\\"Fast responders\\\" were ASA II vs ASA I (OR 2.0, CI 1.1-3.6), ASA III-IV vs ASA I (OR 3.0, CI 1.6-5.5), Walch A1 vs B2 (OR 2.1, CI 1.3-3.3), previous shoulder surgeries (OR 1.8, CI 1.3-2.4), most vs medium socioeconomic deprivation (OR 1.5, CI 1.2-2.0), RTSA for OA vs ATSA for OA (OR 1.8, CI 1.2-2.7), and RTSA for cuff arthropathy or rupture vs ATSA for OA (OR 2.3, CI 1.5-3.4).</p><p><strong>Conclusion: </strong>3 recovery trajectories were identified following TSA, which we labelled as \\\"Fast responders,\\\" \\\"Steady responders,\\\" and \\\"Poor responders.\\\" \\\"Steady responders\\\" and \\\"Poor responders\\\" were more likely to have higher ASA scores, a Walch A1 vs B2 classification, and greater vs medium socioeconomic deprivation than \\\"Fast responders.\\\" Moreover, \\\"Steady responders\\\" were more likely to be female, while \\\"Poor responders\\\" were more likely to have previous shoulder surgeries and RTSA for OA or for cuff arthropathy or rupture than \\\"Fast responders.\\\"</p>\",\"PeriodicalId\":6916,\"journal\":{\"name\":\"Acta Orthopaedica\",\"volume\":\"96 \",\"pages\":\"226-234\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-03-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11881023/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Orthopaedica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2340/17453674.2025.43085\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Orthopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2340/17453674.2025.43085","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:一些患者在全肩关节置换术(TSA)后没有改善,表明不同的恢复轨迹。我们的目的是根据牛津肩部评分(OSS)确定TSA后的恢复轨迹。其次,我们调查了恢复轨迹是否与患者或手术特征相关。方法:我们纳入了2016年至2022年期间在荷兰关节成形术登记册(n = 3,358)中登记的骨关节炎(OA)或袖带病变/破裂术前、术后3个月和/或12个月OSS的原发性解剖性和反转性tsa (atsa /RTSAs)。我们使用潜在类别增长模型(LCGM)来确定恢复模式,并使用多项逻辑回归分析来调查潜在风险因素与类别成员之间的关系(优势比[OR], 95%置信区间[CI])。结果:我们确定了3种恢复模式:“快速反应”(59%),“稳定反应”(27%)和“不良反应”(14%)。与“稳定反应者”和“快速反应者”相关的因素是女性vs男性(OR 2.0, CI 1.5-2.7), ASA III-IV vs ASA I (OR 1.9, CI 1.2-3.1), Walch A1 vs B2 (OR 1.6, CI 1.1-2.5),以及大多数vs中等社会经济剥夺(OR 1.4, CI 1.1-1.9)。“不良反应者”与“快速反应者”相关的因素有ASA II vs ASA I (OR 2.0, CI 1.1-3.6)、ASA III-IV vs ASA I (OR 3.0, CI 1.6-5.5)、Walch A1 vs B2 (OR 2.1, CI 1.3-3.3)、既往肩部手术(OR 1.8, CI 1.3-2.4)、大多数vs中等社会经济剥夺(OR 1.5, CI 1.2-2.0)、OA的RTSA vs OA的ATSA (OR 1.8, CI 1.2-2.7)、袖带关节病或破裂的RTSA vs OA的ATSA (OR 2.3, CI 1.5-3.4)。结论:TSA后确定了3种恢复轨迹,我们将其标记为“快速反应者”,“稳定反应者”和“不良反应者”。与“快速反应者”相比,“稳定反应者”和“不良反应者”更有可能获得更高的ASA分数,Walch A1和B2分类,以及更严重和中等的社会经济剥夺。此外,“稳定反应者”更有可能是女性,而“不良反应者”比“快速反应者”更有可能有过肩关节手术和骨关节炎、袖带关节病或破裂的RTSA。
Identifying recovery trajectories following primary total shoulder arthroplasty: a cohort study of 3,358 patients from the Dutch Arthroplasty Register.
Background and purpose: Some patients do not improve after total shoulder arthroplasty (TSA), indicating different recovery trajectories. We aimed to identify recovery trajectories after TSA based on the Oxford Shoulder Score (OSS). Second, we investigated whether recovery trajectories were associated with patient or procedure characteristics.
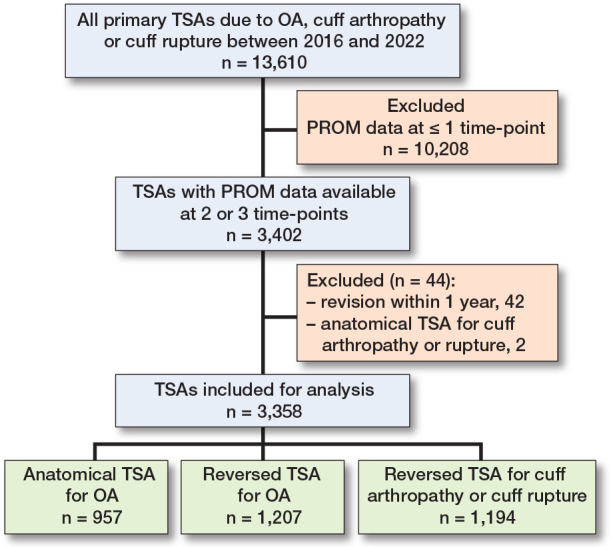
Methods: We included primary anatomical and reversed TSAs (ATSAs/RTSAs) for osteoarthritis (OA) or cuff arthropathy/rupture with preoperative, 3-month, and/or 12-month postoperative OSS, registered between 2016 and 2022 in the Dutch Arthroplasty Register (n = 3,358). We used latent class growth modeling (LCGM) to identify recovery patterns, and multinomial logistic regression analyses to investigate associations between potential risk factors and class membership (odds ratio [OR], 95% confidence interval [CI]).
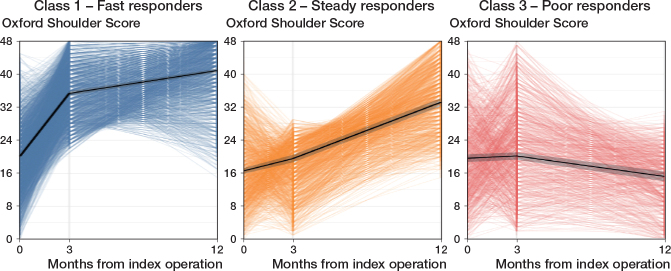
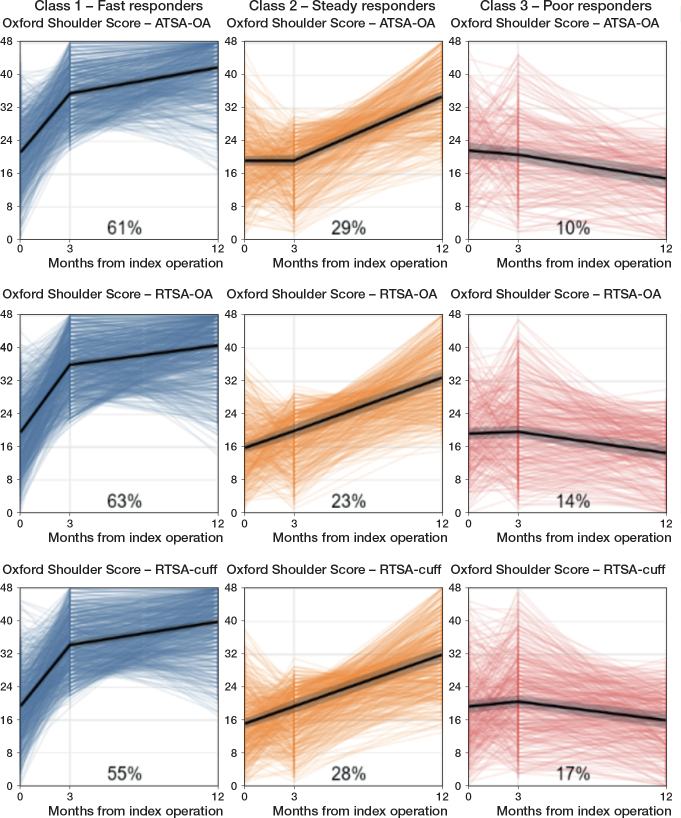
Results: We identified 3 recovery patterns: "Fast responders" (59%), "Steady responders" (27%), and "Poor responders" (14%). Factors associated with "Steady responders" vs "Fast responders" were female vs male sex (OR 2.0, CI 1.5-2.7), ASA III-IV vs ASA I (OR 1.9, CI 1.2-3.1), Walch A1 vs B2 (OR 1.6, CI 1.1-2.5), and most vs medium socioeconomic deprivation (OR 1.4, CI 1.1-1.9). Factors associated with "Poor responders" vs "Fast responders" were ASA II vs ASA I (OR 2.0, CI 1.1-3.6), ASA III-IV vs ASA I (OR 3.0, CI 1.6-5.5), Walch A1 vs B2 (OR 2.1, CI 1.3-3.3), previous shoulder surgeries (OR 1.8, CI 1.3-2.4), most vs medium socioeconomic deprivation (OR 1.5, CI 1.2-2.0), RTSA for OA vs ATSA for OA (OR 1.8, CI 1.2-2.7), and RTSA for cuff arthropathy or rupture vs ATSA for OA (OR 2.3, CI 1.5-3.4).
Conclusion: 3 recovery trajectories were identified following TSA, which we labelled as "Fast responders," "Steady responders," and "Poor responders." "Steady responders" and "Poor responders" were more likely to have higher ASA scores, a Walch A1 vs B2 classification, and greater vs medium socioeconomic deprivation than "Fast responders." Moreover, "Steady responders" were more likely to be female, while "Poor responders" were more likely to have previous shoulder surgeries and RTSA for OA or for cuff arthropathy or rupture than "Fast responders."
期刊介绍:
Acta Orthopaedica (previously Acta Orthopaedica Scandinavica) presents original articles of basic research interest, as well as clinical studies in the field of orthopedics and related sub disciplines. Ever since the journal was founded in 1930, by a group of Scandinavian orthopedic surgeons, the journal has been published for an international audience. Acta Orthopaedica is owned by the Nordic Orthopaedic Federation and is the official publication of this federation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


