Olav Lutro, Marianne Bollestad Tjørhom, Tesfaye Hordofa Leta, Jan-Erik Gjertsen, Geir Hallan, Trond Bruun, Marianne Westberg, Tina Strømdal Wik, Christian Thomas Pollmann, Stein Håkon Lygre, Ove Furnes, Lars Engesæter, Håvard Dale
{"title":"原发性髋关节和膝关节置换术中应该使用多少剂量和哪种类型的抗生素作为系统性抗生素预防?2005-2023年挪威301204例原发性全髋关节、半髋关节和全膝关节置换术的基于登记的研究。","authors":"Olav Lutro, Marianne Bollestad Tjørhom, Tesfaye Hordofa Leta, Jan-Erik Gjertsen, Geir Hallan, Trond Bruun, Marianne Westberg, Tina Strømdal Wik, Christian Thomas Pollmann, Stein Håkon Lygre, Ove Furnes, Lars Engesæter, Håvard Dale","doi":"10.2340/17453674.2025.43003","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Guidelines for systemic antibiotic prophylaxis (SAP) in arthroplasty surgery vary worldwide from repeated doses to only 1 preoperatively. We aimed to investigate, primarily whether 4 doses reduced the risk of PJI compared with 1 to 3 doses, and secondarily if there was a difference between types of antibiotics.</p><p><strong>Methods: </strong>Patients reported to the Norwegian Arthroplasty Register and the Norwegian Hip Fracture Register with primary total knee (TKA), total (THA) or hemi- (HA) hip arthroplasty between 2005 and 2023 were included. Cases with 1 to 4 doses of cefalotin (half-life = 45 minutes), cefazolin (90 minutes), cefuroxime (70 minutes), cloxacillin (30 minutes), or clindamycin (180 minutes) were assessed. Primary outcome was 1-year risk of reoperation (adjusted hazard rate ratio; aHRR) for PJI and was estimated by Cox regression analyses. Secondary outcomes were reoperation for PJI and reoperation for any cause with follow-up of up to 19 years. Non-inferiority analyses and propensity score matching with subsequent Kaplan-Meier analyses were performed with a predetermined non-inferiority margin of 15% (aHRR = 1.15).</p><p><strong>Results: </strong>301,204 cases were included. Of these, 3,388 (1.1%) were reoperated on for PJI within 1 year. The 1-year incidence of reoperation for PJI was 98/9,760 (1.0%) for 1 dose of SAP, 109/10,956 (0.9%) for 2 doses, 178/18,948 (0.9 %) for 3 doses, and 3,003/261,540 (1.0%) for 4 doses. The 1-year risk (aHRR, 95% confidence interval [CI]) of reoperation for PJI was 1.0 (CI 0.8-1.2), 0.9 (CI 0.8-1.2), and 0.9 (CI 0.9-1.1) for 1, 2, and 3 doses, respectively, compared with 4 doses. The 1-year incidence of reoperation for PJI was 2,162/183,964 (1.2%) for cefalotin, 993/91,159 (1.1%) for cefazolin, 35/4,435 (0.8%) for cefuroxime, 85/9,022 (0.9%) for cloxacillin, and 113/12,624 (0.9%) for clindamycin. Compared with cefazolin, cloxacillin (1.2, CI 1.0-1.6) and cefalotin (1.4, CI 1.2-1.5) had a higher risk of reoperation for PJI, whereas cefuroxime (1.0, CI 0.7-1.4) and clindamycin (1.1, CI 0.9-1.3) had a similar risk.</p><p><strong>Conclusion: </strong>4 doses of SAP did not reduce the risk of PJI compared with 1 to 3 doses in primary arthroplasty as measured against PJI. Cefazolin, the 1st-generation cephalosporin with the longest half-life, showed the lowest risk of PJI.</p>","PeriodicalId":6916,"journal":{"name":"Acta Orthopaedica","volume":"96 ","pages":"217-225"},"PeriodicalIF":2.4000,"publicationDate":"2025-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11881024/pdf/","citationCount":"0","resultStr":"{\"title\":\"How many doses and what type of antibiotic should be used as systemic antibiotic prophylaxis in primary hip and knee arthroplasty? A register-based study on 301,204 primary total and hemi- hip and total knee arthroplasties in Norway 2005-2023.\",\"authors\":\"Olav Lutro, Marianne Bollestad Tjørhom, Tesfaye Hordofa Leta, Jan-Erik Gjertsen, Geir Hallan, Trond Bruun, Marianne Westberg, Tina Strømdal Wik, Christian Thomas Pollmann, Stein Håkon Lygre, Ove Furnes, Lars Engesæter, Håvard Dale\",\"doi\":\"10.2340/17453674.2025.43003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and purpose: </strong>Guidelines for systemic antibiotic prophylaxis (SAP) in arthroplasty surgery vary worldwide from repeated doses to only 1 preoperatively. We aimed to investigate, primarily whether 4 doses reduced the risk of PJI compared with 1 to 3 doses, and secondarily if there was a difference between types of antibiotics.</p><p><strong>Methods: </strong>Patients reported to the Norwegian Arthroplasty Register and the Norwegian Hip Fracture Register with primary total knee (TKA), total (THA) or hemi- (HA) hip arthroplasty between 2005 and 2023 were included. Cases with 1 to 4 doses of cefalotin (half-life = 45 minutes), cefazolin (90 minutes), cefuroxime (70 minutes), cloxacillin (30 minutes), or clindamycin (180 minutes) were assessed. Primary outcome was 1-year risk of reoperation (adjusted hazard rate ratio; aHRR) for PJI and was estimated by Cox regression analyses. Secondary outcomes were reoperation for PJI and reoperation for any cause with follow-up of up to 19 years. Non-inferiority analyses and propensity score matching with subsequent Kaplan-Meier analyses were performed with a predetermined non-inferiority margin of 15% (aHRR = 1.15).</p><p><strong>Results: </strong>301,204 cases were included. Of these, 3,388 (1.1%) were reoperated on for PJI within 1 year. The 1-year incidence of reoperation for PJI was 98/9,760 (1.0%) for 1 dose of SAP, 109/10,956 (0.9%) for 2 doses, 178/18,948 (0.9 %) for 3 doses, and 3,003/261,540 (1.0%) for 4 doses. The 1-year risk (aHRR, 95% confidence interval [CI]) of reoperation for PJI was 1.0 (CI 0.8-1.2), 0.9 (CI 0.8-1.2), and 0.9 (CI 0.9-1.1) for 1, 2, and 3 doses, respectively, compared with 4 doses. The 1-year incidence of reoperation for PJI was 2,162/183,964 (1.2%) for cefalotin, 993/91,159 (1.1%) for cefazolin, 35/4,435 (0.8%) for cefuroxime, 85/9,022 (0.9%) for cloxacillin, and 113/12,624 (0.9%) for clindamycin. Compared with cefazolin, cloxacillin (1.2, CI 1.0-1.6) and cefalotin (1.4, CI 1.2-1.5) had a higher risk of reoperation for PJI, whereas cefuroxime (1.0, CI 0.7-1.4) and clindamycin (1.1, CI 0.9-1.3) had a similar risk.</p><p><strong>Conclusion: </strong>4 doses of SAP did not reduce the risk of PJI compared with 1 to 3 doses in primary arthroplasty as measured against PJI. Cefazolin, the 1st-generation cephalosporin with the longest half-life, showed the lowest risk of PJI.</p>\",\"PeriodicalId\":6916,\"journal\":{\"name\":\"Acta Orthopaedica\",\"volume\":\"96 \",\"pages\":\"217-225\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-03-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11881024/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Orthopaedica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2340/17453674.2025.43003\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Orthopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2340/17453674.2025.43003","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
How many doses and what type of antibiotic should be used as systemic antibiotic prophylaxis in primary hip and knee arthroplasty? A register-based study on 301,204 primary total and hemi- hip and total knee arthroplasties in Norway 2005-2023.
Background and purpose: Guidelines for systemic antibiotic prophylaxis (SAP) in arthroplasty surgery vary worldwide from repeated doses to only 1 preoperatively. We aimed to investigate, primarily whether 4 doses reduced the risk of PJI compared with 1 to 3 doses, and secondarily if there was a difference between types of antibiotics.
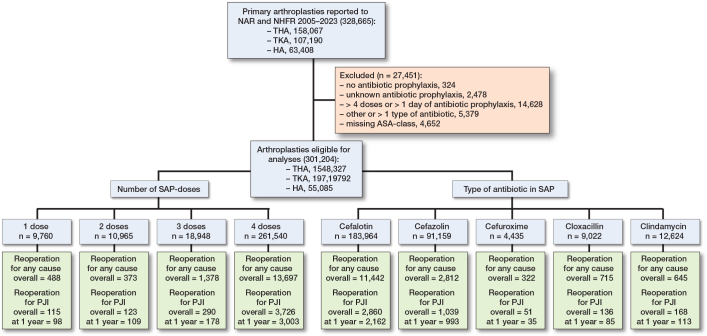
Methods: Patients reported to the Norwegian Arthroplasty Register and the Norwegian Hip Fracture Register with primary total knee (TKA), total (THA) or hemi- (HA) hip arthroplasty between 2005 and 2023 were included. Cases with 1 to 4 doses of cefalotin (half-life = 45 minutes), cefazolin (90 minutes), cefuroxime (70 minutes), cloxacillin (30 minutes), or clindamycin (180 minutes) were assessed. Primary outcome was 1-year risk of reoperation (adjusted hazard rate ratio; aHRR) for PJI and was estimated by Cox regression analyses. Secondary outcomes were reoperation for PJI and reoperation for any cause with follow-up of up to 19 years. Non-inferiority analyses and propensity score matching with subsequent Kaplan-Meier analyses were performed with a predetermined non-inferiority margin of 15% (aHRR = 1.15).
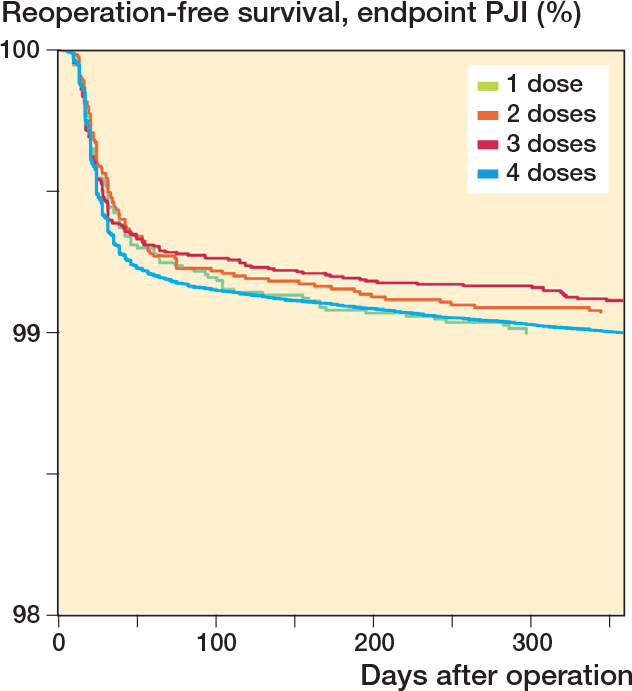
Results: 301,204 cases were included. Of these, 3,388 (1.1%) were reoperated on for PJI within 1 year. The 1-year incidence of reoperation for PJI was 98/9,760 (1.0%) for 1 dose of SAP, 109/10,956 (0.9%) for 2 doses, 178/18,948 (0.9 %) for 3 doses, and 3,003/261,540 (1.0%) for 4 doses. The 1-year risk (aHRR, 95% confidence interval [CI]) of reoperation for PJI was 1.0 (CI 0.8-1.2), 0.9 (CI 0.8-1.2), and 0.9 (CI 0.9-1.1) for 1, 2, and 3 doses, respectively, compared with 4 doses. The 1-year incidence of reoperation for PJI was 2,162/183,964 (1.2%) for cefalotin, 993/91,159 (1.1%) for cefazolin, 35/4,435 (0.8%) for cefuroxime, 85/9,022 (0.9%) for cloxacillin, and 113/12,624 (0.9%) for clindamycin. Compared with cefazolin, cloxacillin (1.2, CI 1.0-1.6) and cefalotin (1.4, CI 1.2-1.5) had a higher risk of reoperation for PJI, whereas cefuroxime (1.0, CI 0.7-1.4) and clindamycin (1.1, CI 0.9-1.3) had a similar risk.
Conclusion: 4 doses of SAP did not reduce the risk of PJI compared with 1 to 3 doses in primary arthroplasty as measured against PJI. Cefazolin, the 1st-generation cephalosporin with the longest half-life, showed the lowest risk of PJI.
期刊介绍:
Acta Orthopaedica (previously Acta Orthopaedica Scandinavica) presents original articles of basic research interest, as well as clinical studies in the field of orthopedics and related sub disciplines. Ever since the journal was founded in 1930, by a group of Scandinavian orthopedic surgeons, the journal has been published for an international audience. Acta Orthopaedica is owned by the Nordic Orthopaedic Federation and is the official publication of this federation.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


