Juan Schmukler, Tengfei Li, Joel A Block, Theodore Pincus
{"title":"风湿病医师0 - 10在现代风湿病护理的初始与随访中对炎症、损伤和患者窘迫的评估。","authors":"Juan Schmukler, Tengfei Li, Joel A Block, Theodore Pincus","doi":"10.1002/acr2.70010","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We aimed to analyze the RheuMetric physician 0 to 10 visual numeric subscale (VNS) estimates of inflammatory activity (DOCINF), organ damage (DOCDAM), and patient distress (DOCDIS) at initial and follow-up routine rheumatology visits for possible incremental information to clarify physician estimate of global assessment (DOCGL).</p><p><strong>Methods: </strong>A retrospective cross-sectional study compared mean DOCGL, DOCINF, DOCDAM, and DOCDIS and the percentage contributed by inflammation, damage, and distress to DOCGL (total = 100%) at initial and follow-up visits in 563 unselected routine care patients, classified into four diagnosis categories: inflammatory (rheumatoid arthritis, systemic lupus erythematosus [SLE], spondylarthritis, vasculitis, and gout), primary osteoarthritis (OA), primary fibromyalgia (FM), and \"other\" diagnoses. Differences between initial and follow-up visits were estimated using t-tests.</p><p><strong>Results: </strong>In all patients, mean DOCGL was 4.0/10, DOCINF 1.6/10, DOCDAM 2.9/10, and DOCDIS 2.4/10, indicating higher estimates for damage and distress than for inflammation, including in all inflammatory diagnoses other than SLE. Highest mean estimates were 2.2 for DOCINF in inflammatory diagnoses, 4.9 for DOCDAM in primary OA, 6.3 for DOCDIS in primary FM. However, DOCDAM was 2.8 (0.6 uniyts higher than DOCINF) in inflammatory diagnoses. RheuMetric estimates of inflammation were significantly higher at initial than at follow-up visits, and estimates of damage were significantly lower at initial than at follow-up visits in all patients and in those with inflammatory diagnoses. DOCGL did not differ significantly at initial versus follow-up visits.</p><p><strong>Conclusion: </strong>DOCINF, DOCDAM, and DOCDIS add feasibly recorded, clinically relevant incremental information to DOCGL. Despite excellent contemporary control of inflammation, joint damage and patient distress remain important clinical problems in contemporary routine rheumatology care, documented by quantitative RheuMetric estimates.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 3","pages":"e70010"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11877136/pdf/","citationCount":"0","resultStr":"{\"title\":\"RheuMetric Physician 0 to 10 Estimates of Inflammation, Damage, and Patient Distress at Initial Versus Follow-Up Visits in Contemporary Rheumatology Care.\",\"authors\":\"Juan Schmukler, Tengfei Li, Joel A Block, Theodore Pincus\",\"doi\":\"10.1002/acr2.70010\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>We aimed to analyze the RheuMetric physician 0 to 10 visual numeric subscale (VNS) estimates of inflammatory activity (DOCINF), organ damage (DOCDAM), and patient distress (DOCDIS) at initial and follow-up routine rheumatology visits for possible incremental information to clarify physician estimate of global assessment (DOCGL).</p><p><strong>Methods: </strong>A retrospective cross-sectional study compared mean DOCGL, DOCINF, DOCDAM, and DOCDIS and the percentage contributed by inflammation, damage, and distress to DOCGL (total = 100%) at initial and follow-up visits in 563 unselected routine care patients, classified into four diagnosis categories: inflammatory (rheumatoid arthritis, systemic lupus erythematosus [SLE], spondylarthritis, vasculitis, and gout), primary osteoarthritis (OA), primary fibromyalgia (FM), and \\\"other\\\" diagnoses. Differences between initial and follow-up visits were estimated using t-tests.</p><p><strong>Results: </strong>In all patients, mean DOCGL was 4.0/10, DOCINF 1.6/10, DOCDAM 2.9/10, and DOCDIS 2.4/10, indicating higher estimates for damage and distress than for inflammation, including in all inflammatory diagnoses other than SLE. Highest mean estimates were 2.2 for DOCINF in inflammatory diagnoses, 4.9 for DOCDAM in primary OA, 6.3 for DOCDIS in primary FM. However, DOCDAM was 2.8 (0.6 uniyts higher than DOCINF) in inflammatory diagnoses. RheuMetric estimates of inflammation were significantly higher at initial than at follow-up visits, and estimates of damage were significantly lower at initial than at follow-up visits in all patients and in those with inflammatory diagnoses. DOCGL did not differ significantly at initial versus follow-up visits.</p><p><strong>Conclusion: </strong>DOCINF, DOCDAM, and DOCDIS add feasibly recorded, clinically relevant incremental information to DOCGL. Despite excellent contemporary control of inflammation, joint damage and patient distress remain important clinical problems in contemporary routine rheumatology care, documented by quantitative RheuMetric estimates.</p>\",\"PeriodicalId\":93845,\"journal\":{\"name\":\"ACR open rheumatology\",\"volume\":\"7 3\",\"pages\":\"e70010\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11877136/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR open rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.70010\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
RheuMetric Physician 0 to 10 Estimates of Inflammation, Damage, and Patient Distress at Initial Versus Follow-Up Visits in Contemporary Rheumatology Care.
Objective: We aimed to analyze the RheuMetric physician 0 to 10 visual numeric subscale (VNS) estimates of inflammatory activity (DOCINF), organ damage (DOCDAM), and patient distress (DOCDIS) at initial and follow-up routine rheumatology visits for possible incremental information to clarify physician estimate of global assessment (DOCGL).
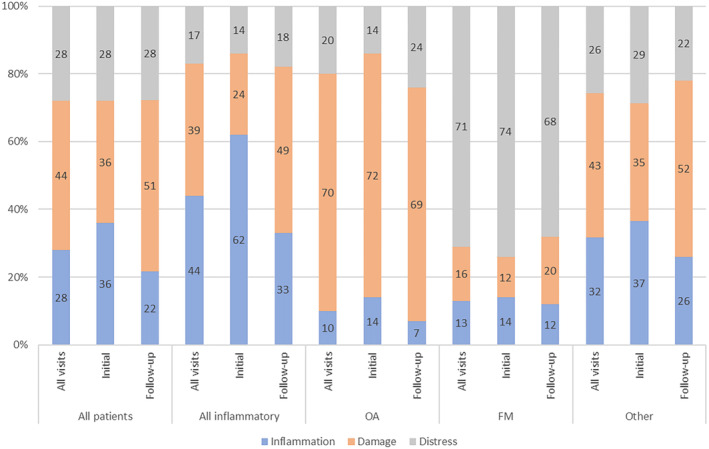
Methods: A retrospective cross-sectional study compared mean DOCGL, DOCINF, DOCDAM, and DOCDIS and the percentage contributed by inflammation, damage, and distress to DOCGL (total = 100%) at initial and follow-up visits in 563 unselected routine care patients, classified into four diagnosis categories: inflammatory (rheumatoid arthritis, systemic lupus erythematosus [SLE], spondylarthritis, vasculitis, and gout), primary osteoarthritis (OA), primary fibromyalgia (FM), and "other" diagnoses. Differences between initial and follow-up visits were estimated using t-tests.
Results: In all patients, mean DOCGL was 4.0/10, DOCINF 1.6/10, DOCDAM 2.9/10, and DOCDIS 2.4/10, indicating higher estimates for damage and distress than for inflammation, including in all inflammatory diagnoses other than SLE. Highest mean estimates were 2.2 for DOCINF in inflammatory diagnoses, 4.9 for DOCDAM in primary OA, 6.3 for DOCDIS in primary FM. However, DOCDAM was 2.8 (0.6 uniyts higher than DOCINF) in inflammatory diagnoses. RheuMetric estimates of inflammation were significantly higher at initial than at follow-up visits, and estimates of damage were significantly lower at initial than at follow-up visits in all patients and in those with inflammatory diagnoses. DOCGL did not differ significantly at initial versus follow-up visits.
Conclusion: DOCINF, DOCDAM, and DOCDIS add feasibly recorded, clinically relevant incremental information to DOCGL. Despite excellent contemporary control of inflammation, joint damage and patient distress remain important clinical problems in contemporary routine rheumatology care, documented by quantitative RheuMetric estimates.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


