Jiha Lee, Jonathan Martindale, Beth I Wallace, Namrata Singh, Una E Makris, Julie P W Bynum
{"title":"新诊断为晚发性类风湿关节炎的老年人长期糖皮质激素使用的变化","authors":"Jiha Lee, Jonathan Martindale, Beth I Wallace, Namrata Singh, Una E Makris, Julie P W Bynum","doi":"10.1002/acr2.70013","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We evaluated changes in long-term glucocorticoid (GC) use and factors associated with persistent GC use in older adults with late-onset rheumatoid arthritis (LORA).</p><p><strong>Methods: </strong>Using 20% Medicare data from 2008 to 2017, we identified adults ≥66 years with a new diagnosis of LORA, disease-modifying antirheumatic drug (DMARD) use or at least two rheumatologist visits, and at least 12 months of follow-up data. Older adults were categorized as DMARD-exposed or DMARD-unexposed based on treatment during the 12 months after LORA diagnosis (index date). For each quarter after the index date, long-term GC use was defined as having oral GC prescriptions for at least 30 days with a dose >5 mg/day prednisone equivalent. We compared long-term GC use between quarter (Q)1 and Q4 and performed stratified mixed-effects logistic regression for factors associated with persistent GC use, defined as long-term GC use in Q2 to Q4.</p><p><strong>Results: </strong>The cohort included 15,425 individuals with two-thirds (62.5%) being DMARD-exposed. Between Q1 and Q4, the proportion of older adults on long-term GC declined from 44.1 to 24.9% (∆19.2%) among the DMARD-exposed and from 25.8 to 17.9% (∆7.9%) among the DMARD-unexposed. One year after the index date, 13.5% of the DMARD-exposed and 9.8% of the DMARD-unexposed were persistent GC users. In stratified mixed-effects logistic models, persistent GC use was associated with low-income subsidy status among the DMARD-exposed and with greater comorbidity burden among DMARD-unexposed.</p><p><strong>Conclusion: </strong>Long-term GC use declined more among DMARD-exposed than DMARD-unexposed patients. One in seven DMARD-exposed and one in ten DMARD-unexposed have persistent GC use which is associated with financial barriers and multimorbidity that may limit the use of steroid-sparing DMARDs.</p>","PeriodicalId":93845,"journal":{"name":"ACR open rheumatology","volume":"7 3","pages":"e70013"},"PeriodicalIF":2.8000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11877135/pdf/","citationCount":"0","resultStr":"{\"title\":\"Changes in Long-Term Glucocorticoid Use Among Older Adults After New Diagnosis of Late-Onset Rheumatoid Arthritis.\",\"authors\":\"Jiha Lee, Jonathan Martindale, Beth I Wallace, Namrata Singh, Una E Makris, Julie P W Bynum\",\"doi\":\"10.1002/acr2.70013\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>We evaluated changes in long-term glucocorticoid (GC) use and factors associated with persistent GC use in older adults with late-onset rheumatoid arthritis (LORA).</p><p><strong>Methods: </strong>Using 20% Medicare data from 2008 to 2017, we identified adults ≥66 years with a new diagnosis of LORA, disease-modifying antirheumatic drug (DMARD) use or at least two rheumatologist visits, and at least 12 months of follow-up data. Older adults were categorized as DMARD-exposed or DMARD-unexposed based on treatment during the 12 months after LORA diagnosis (index date). For each quarter after the index date, long-term GC use was defined as having oral GC prescriptions for at least 30 days with a dose >5 mg/day prednisone equivalent. We compared long-term GC use between quarter (Q)1 and Q4 and performed stratified mixed-effects logistic regression for factors associated with persistent GC use, defined as long-term GC use in Q2 to Q4.</p><p><strong>Results: </strong>The cohort included 15,425 individuals with two-thirds (62.5%) being DMARD-exposed. Between Q1 and Q4, the proportion of older adults on long-term GC declined from 44.1 to 24.9% (∆19.2%) among the DMARD-exposed and from 25.8 to 17.9% (∆7.9%) among the DMARD-unexposed. One year after the index date, 13.5% of the DMARD-exposed and 9.8% of the DMARD-unexposed were persistent GC users. In stratified mixed-effects logistic models, persistent GC use was associated with low-income subsidy status among the DMARD-exposed and with greater comorbidity burden among DMARD-unexposed.</p><p><strong>Conclusion: </strong>Long-term GC use declined more among DMARD-exposed than DMARD-unexposed patients. One in seven DMARD-exposed and one in ten DMARD-unexposed have persistent GC use which is associated with financial barriers and multimorbidity that may limit the use of steroid-sparing DMARDs.</p>\",\"PeriodicalId\":93845,\"journal\":{\"name\":\"ACR open rheumatology\",\"volume\":\"7 3\",\"pages\":\"e70013\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11877135/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR open rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.70013\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR open rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.70013","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Changes in Long-Term Glucocorticoid Use Among Older Adults After New Diagnosis of Late-Onset Rheumatoid Arthritis.
Background: We evaluated changes in long-term glucocorticoid (GC) use and factors associated with persistent GC use in older adults with late-onset rheumatoid arthritis (LORA).
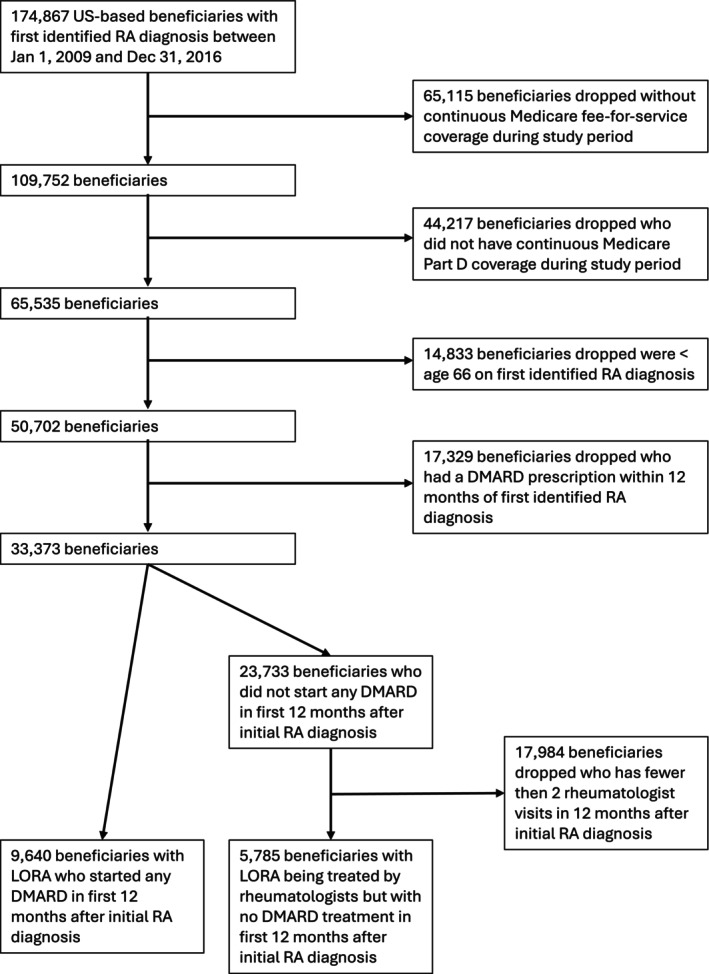
Methods: Using 20% Medicare data from 2008 to 2017, we identified adults ≥66 years with a new diagnosis of LORA, disease-modifying antirheumatic drug (DMARD) use or at least two rheumatologist visits, and at least 12 months of follow-up data. Older adults were categorized as DMARD-exposed or DMARD-unexposed based on treatment during the 12 months after LORA diagnosis (index date). For each quarter after the index date, long-term GC use was defined as having oral GC prescriptions for at least 30 days with a dose >5 mg/day prednisone equivalent. We compared long-term GC use between quarter (Q)1 and Q4 and performed stratified mixed-effects logistic regression for factors associated with persistent GC use, defined as long-term GC use in Q2 to Q4.
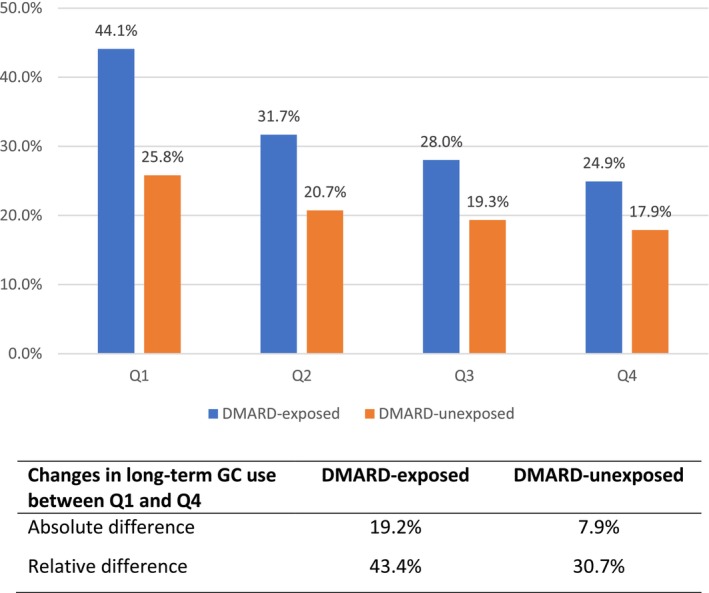
Results: The cohort included 15,425 individuals with two-thirds (62.5%) being DMARD-exposed. Between Q1 and Q4, the proportion of older adults on long-term GC declined from 44.1 to 24.9% (∆19.2%) among the DMARD-exposed and from 25.8 to 17.9% (∆7.9%) among the DMARD-unexposed. One year after the index date, 13.5% of the DMARD-exposed and 9.8% of the DMARD-unexposed were persistent GC users. In stratified mixed-effects logistic models, persistent GC use was associated with low-income subsidy status among the DMARD-exposed and with greater comorbidity burden among DMARD-unexposed.
Conclusion: Long-term GC use declined more among DMARD-exposed than DMARD-unexposed patients. One in seven DMARD-exposed and one in ten DMARD-unexposed have persistent GC use which is associated with financial barriers and multimorbidity that may limit the use of steroid-sparing DMARDs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


