Adri M Durant, Mimi Nguyen, Mouneeb M Choudry, Lanyu Mi, Jack R Andrews, Mark D Tyson
{"title":"大容量高级别非浸润性膀胱癌重复TURBT。","authors":"Adri M Durant, Mimi Nguyen, Mouneeb M Choudry, Lanyu Mi, Jack R Andrews, Mark D Tyson","doi":"10.1177/23523735241303350","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The American Urological Association (AUA)/Society of Urology Oncology (SUO) guidelines recommend a repeat transurethral resection of bladder tumor (TURBT) for high-risk, non-invasive (HR Ta) nonmuscle invasive bladder cancer (NMIBC) patients. The evidence base for this recommendation is weak (grade C) and fraught with methodological shortcomings, such as the lack of adjuvant intravesical Bacillus Calmette Guerin (BCG) and single-center study designs.</p><p><strong>Objective: </strong>We sought to evaluate the effect of repeat TURBT on recurrence-free survival at a population level in HR Ta NMIBC patients who completed BCG induction therapy.</p><p><strong>Methods: </strong>High-grade Ta NMIBC patients who underwent TURBT for a ≥5 cm tumor were identified within the SEER-Medicare database. All patients completed induction BCG and were stratified into two groups: repeat TURBT within eight weeks of initial TURBT and a group without repeat TURBT (control group). The primary endpoint was the 3-year high-risk recurrence rate.</p><p><strong>Results: </strong>A cohort of 604 patients was identified, with 93 (15.4%) undergoing a repeat TURBT within eight weeks of initial TURBT and 511 (84.6%) without a repeat TURBT. Patient demographic and clinical characteristics were similar overall. No significant difference in the 3-year recurrence rate was noted (repeat TURBT: 20.4% vs. control group: 15.7%, p = 0.25). After adjusting for demographic and clinical characteristics, no association between repeat TURBT and 3-year high-risk recurrence was observed (HR (95% CI): 1.27 (0.76, 2.11); p = 0.36).</p><p><strong>Conclusion: </strong>Although our study contains several major limitations, our results suggest that repeat TURBT in large volume HG Ta NMIBC treated with induction BCG therapy was not associated with improved high-risk recurrence-free survival.</p>","PeriodicalId":54217,"journal":{"name":"Bladder Cancer","volume":"10 4","pages":"270-277"},"PeriodicalIF":1.2000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11864239/pdf/","citationCount":"0","resultStr":"{\"title\":\"Repeat TURBT in large volume high-grade non-invasive bladder cancer.\",\"authors\":\"Adri M Durant, Mimi Nguyen, Mouneeb M Choudry, Lanyu Mi, Jack R Andrews, Mark D Tyson\",\"doi\":\"10.1177/23523735241303350\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The American Urological Association (AUA)/Society of Urology Oncology (SUO) guidelines recommend a repeat transurethral resection of bladder tumor (TURBT) for high-risk, non-invasive (HR Ta) nonmuscle invasive bladder cancer (NMIBC) patients. The evidence base for this recommendation is weak (grade C) and fraught with methodological shortcomings, such as the lack of adjuvant intravesical Bacillus Calmette Guerin (BCG) and single-center study designs.</p><p><strong>Objective: </strong>We sought to evaluate the effect of repeat TURBT on recurrence-free survival at a population level in HR Ta NMIBC patients who completed BCG induction therapy.</p><p><strong>Methods: </strong>High-grade Ta NMIBC patients who underwent TURBT for a ≥5 cm tumor were identified within the SEER-Medicare database. All patients completed induction BCG and were stratified into two groups: repeat TURBT within eight weeks of initial TURBT and a group without repeat TURBT (control group). The primary endpoint was the 3-year high-risk recurrence rate.</p><p><strong>Results: </strong>A cohort of 604 patients was identified, with 93 (15.4%) undergoing a repeat TURBT within eight weeks of initial TURBT and 511 (84.6%) without a repeat TURBT. Patient demographic and clinical characteristics were similar overall. No significant difference in the 3-year recurrence rate was noted (repeat TURBT: 20.4% vs. control group: 15.7%, p = 0.25). After adjusting for demographic and clinical characteristics, no association between repeat TURBT and 3-year high-risk recurrence was observed (HR (95% CI): 1.27 (0.76, 2.11); p = 0.36).</p><p><strong>Conclusion: </strong>Although our study contains several major limitations, our results suggest that repeat TURBT in large volume HG Ta NMIBC treated with induction BCG therapy was not associated with improved high-risk recurrence-free survival.</p>\",\"PeriodicalId\":54217,\"journal\":{\"name\":\"Bladder Cancer\",\"volume\":\"10 4\",\"pages\":\"270-277\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11864239/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bladder Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/23523735241303350\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bladder Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/23523735241303350","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Repeat TURBT in large volume high-grade non-invasive bladder cancer.
Background: The American Urological Association (AUA)/Society of Urology Oncology (SUO) guidelines recommend a repeat transurethral resection of bladder tumor (TURBT) for high-risk, non-invasive (HR Ta) nonmuscle invasive bladder cancer (NMIBC) patients. The evidence base for this recommendation is weak (grade C) and fraught with methodological shortcomings, such as the lack of adjuvant intravesical Bacillus Calmette Guerin (BCG) and single-center study designs.
Objective: We sought to evaluate the effect of repeat TURBT on recurrence-free survival at a population level in HR Ta NMIBC patients who completed BCG induction therapy.
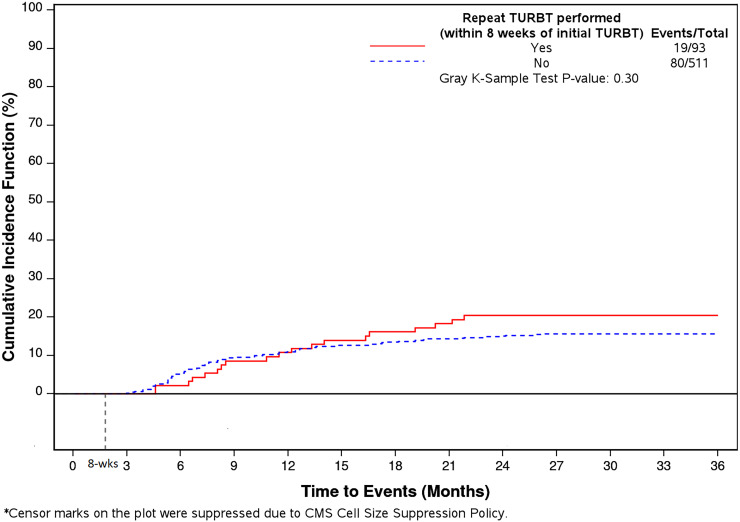
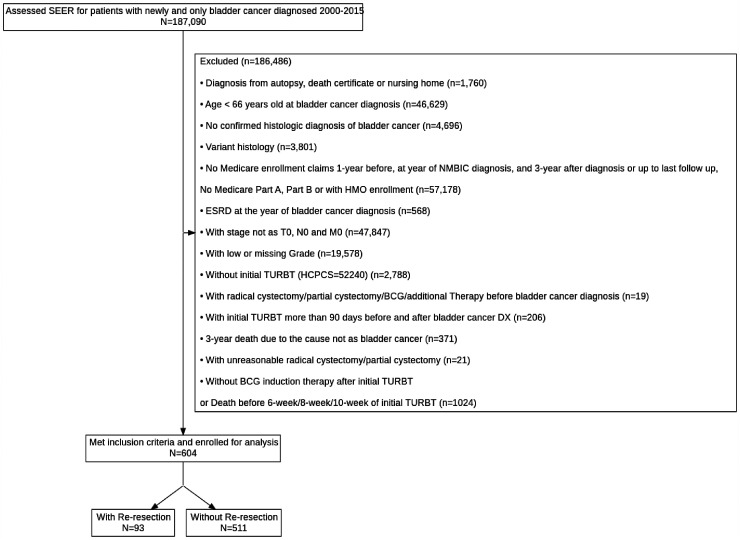
Methods: High-grade Ta NMIBC patients who underwent TURBT for a ≥5 cm tumor were identified within the SEER-Medicare database. All patients completed induction BCG and were stratified into two groups: repeat TURBT within eight weeks of initial TURBT and a group without repeat TURBT (control group). The primary endpoint was the 3-year high-risk recurrence rate.
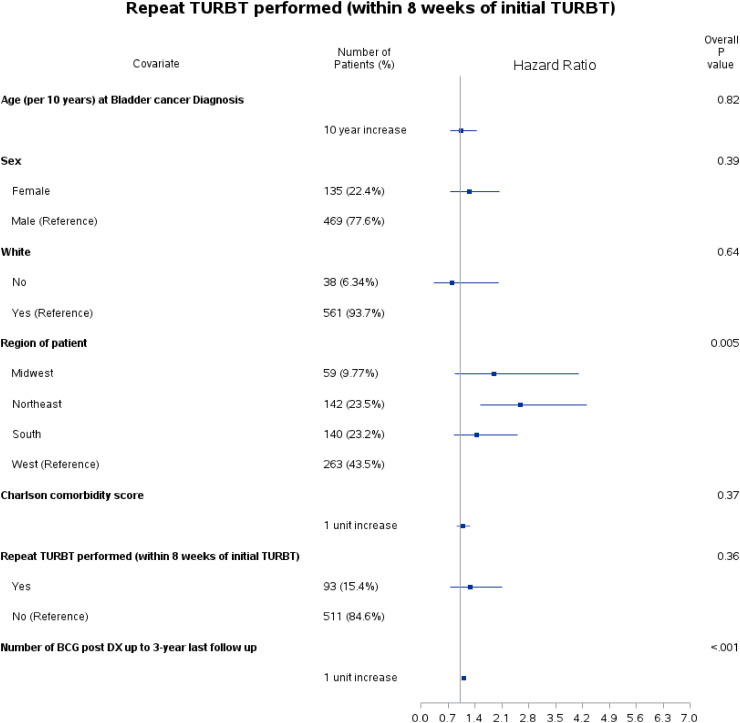
Results: A cohort of 604 patients was identified, with 93 (15.4%) undergoing a repeat TURBT within eight weeks of initial TURBT and 511 (84.6%) without a repeat TURBT. Patient demographic and clinical characteristics were similar overall. No significant difference in the 3-year recurrence rate was noted (repeat TURBT: 20.4% vs. control group: 15.7%, p = 0.25). After adjusting for demographic and clinical characteristics, no association between repeat TURBT and 3-year high-risk recurrence was observed (HR (95% CI): 1.27 (0.76, 2.11); p = 0.36).
Conclusion: Although our study contains several major limitations, our results suggest that repeat TURBT in large volume HG Ta NMIBC treated with induction BCG therapy was not associated with improved high-risk recurrence-free survival.
期刊介绍:
Bladder Cancer is an international multidisciplinary journal to facilitate progress in understanding the epidemiology/etiology, genetics, molecular correlates, pathogenesis, pharmacology, ethics, patient advocacy and survivorship, diagnosis and treatment of tumors of the bladder and upper urinary tract. The journal publishes research reports, reviews, short communications, and letters-to-the-editor. The journal is dedicated to providing an open forum for original research in basic science, translational research and clinical medicine that expedites our fundamental understanding and improves treatment of tumors of the bladder and upper urinary tract.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


