Abhinav Sharma, Paramveer Birring, Nischal Acharya, Manaav Mehta, Nicole Liu Goldenhersh, Michael Steinhaus, Hao-Hua Wu, Sohaib Hashmi, Don Young Park, Yu-Po Lee, Nitin Bhatia
{"title":"与单纯减压相比,减压融合治疗腰椎退行性滑脱的早期发病率和围手术期并发症的风险更高:美国的一项回顾性研究。","authors":"Abhinav Sharma, Paramveer Birring, Nischal Acharya, Manaav Mehta, Nicole Liu Goldenhersh, Michael Steinhaus, Hao-Hua Wu, Sohaib Hashmi, Don Young Park, Yu-Po Lee, Nitin Bhatia","doi":"10.31616/asj.2024.0279","DOIUrl":null,"url":null,"abstract":"<p><strong>Study design: </strong>A retrospective cohort study.</p><p><strong>Purpose: </strong>To assess differences in 30-day morbidity and mortality and postoperative complications between two surgical treatment options.</p><p><strong>Overview of literature: </strong>The choice of decompression with fusion or decompression alone for the management of degenerative spondylolisthesis (DS) is controversial.</p><p><strong>Methods: </strong>The American College of Surgeons National Quality Improvement Program database was queried for laminectomy or laminotomy with and without fusion from 2015 to 2020. The estimated 30-day mortality and morbidity, 30-day complications, and American Society of Anesthesiologist (ASA) classification were evaluated through chi-square and analysis of variance tests, with the results further stratified according to the ASA classification.</p><p><strong>Results: </strong>Of the 4,120 patients, 2,384 (58%) underwent a laminectomy or laminotomy without fusion and 1,736 (42%) underwent a laminectomy or laminotomy with fusion. Patients undergoing decompression with fusion had higher mean mortality (estimated probability 0.0034 vs. 0.0027, p<0.001), mean morbidity (estimated probability 0.053 vs. 0.048, p<0.001), mean length of stay (3.62±3.4 days vs. 3.15±4.3 days, p<0.001), and bleeding risk necessitating transfusion (9.5% vs. 7.6%, p =0.038). There was a higher rate of overall 30-day postoperative complications associated with an increasing ASA score for both cohorts.</p><p><strong>Conclusions: </strong>Decompression with fusion was associated with higher estimated mortality, morbidity, and 30-day complications. Decompression alone is an appealing treatment option for lumbar DS, particularly for patients with higher ASA scores and those at higher risk.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"346-354"},"PeriodicalIF":2.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242256/pdf/","citationCount":"0","resultStr":"{\"title\":\"Decompression and fusion for lumbar degenerative spondylolisthesis is associated with higher early morbidity rates and risk of perioperative complications compared with decompression alone: a retrospective study in the United States.\",\"authors\":\"Abhinav Sharma, Paramveer Birring, Nischal Acharya, Manaav Mehta, Nicole Liu Goldenhersh, Michael Steinhaus, Hao-Hua Wu, Sohaib Hashmi, Don Young Park, Yu-Po Lee, Nitin Bhatia\",\"doi\":\"10.31616/asj.2024.0279\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Study design: </strong>A retrospective cohort study.</p><p><strong>Purpose: </strong>To assess differences in 30-day morbidity and mortality and postoperative complications between two surgical treatment options.</p><p><strong>Overview of literature: </strong>The choice of decompression with fusion or decompression alone for the management of degenerative spondylolisthesis (DS) is controversial.</p><p><strong>Methods: </strong>The American College of Surgeons National Quality Improvement Program database was queried for laminectomy or laminotomy with and without fusion from 2015 to 2020. The estimated 30-day mortality and morbidity, 30-day complications, and American Society of Anesthesiologist (ASA) classification were evaluated through chi-square and analysis of variance tests, with the results further stratified according to the ASA classification.</p><p><strong>Results: </strong>Of the 4,120 patients, 2,384 (58%) underwent a laminectomy or laminotomy without fusion and 1,736 (42%) underwent a laminectomy or laminotomy with fusion. Patients undergoing decompression with fusion had higher mean mortality (estimated probability 0.0034 vs. 0.0027, p<0.001), mean morbidity (estimated probability 0.053 vs. 0.048, p<0.001), mean length of stay (3.62±3.4 days vs. 3.15±4.3 days, p<0.001), and bleeding risk necessitating transfusion (9.5% vs. 7.6%, p =0.038). There was a higher rate of overall 30-day postoperative complications associated with an increasing ASA score for both cohorts.</p><p><strong>Conclusions: </strong>Decompression with fusion was associated with higher estimated mortality, morbidity, and 30-day complications. Decompression alone is an appealing treatment option for lumbar DS, particularly for patients with higher ASA scores and those at higher risk.</p>\",\"PeriodicalId\":8555,\"journal\":{\"name\":\"Asian Spine Journal\",\"volume\":\" \",\"pages\":\"346-354\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12242256/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asian Spine Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31616/asj.2024.0279\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2024.0279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
研究设计:回顾性队列研究。目的:评估两种手术治疗方案在30天发病率、死亡率和术后并发症方面的差异。文献综述:选择减压融合或单独减压治疗退行性椎体滑脱(DS)是有争议的。方法:查询2015年至2020年美国外科医师学会国家质量改进计划数据库中椎板切除术或椎板切除术合并和不合并融合的病例。通过卡方检验和方差分析评估30天死亡率和发病率、30天并发症和美国麻醉医师协会(ASA)分类,并根据ASA分类对结果进一步分层。结果:在4120例患者中,2384例(58%)行椎板切除术或椎板切开术不融合,1736例(42%)行椎板切除术或椎板切开术融合。接受减压融合的患者有更高的平均死亡率(估计概率为0.0034 vs. 0.0027)。结论:减压融合与更高的估计死亡率、发病率和30天并发症相关。单独减压是腰椎退行性滑移的一种有吸引力的治疗选择,特别是对于ASA评分较高和风险较高的患者。
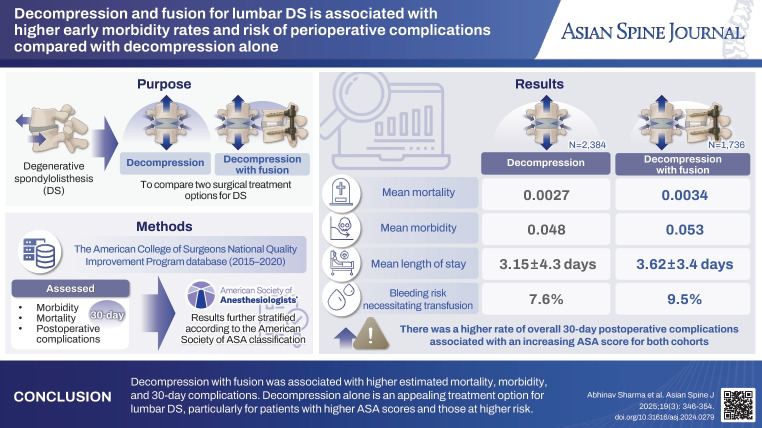
Decompression and fusion for lumbar degenerative spondylolisthesis is associated with higher early morbidity rates and risk of perioperative complications compared with decompression alone: a retrospective study in the United States.
Study design: A retrospective cohort study.
Purpose: To assess differences in 30-day morbidity and mortality and postoperative complications between two surgical treatment options.
Overview of literature: The choice of decompression with fusion or decompression alone for the management of degenerative spondylolisthesis (DS) is controversial.
Methods: The American College of Surgeons National Quality Improvement Program database was queried for laminectomy or laminotomy with and without fusion from 2015 to 2020. The estimated 30-day mortality and morbidity, 30-day complications, and American Society of Anesthesiologist (ASA) classification were evaluated through chi-square and analysis of variance tests, with the results further stratified according to the ASA classification.
Results: Of the 4,120 patients, 2,384 (58%) underwent a laminectomy or laminotomy without fusion and 1,736 (42%) underwent a laminectomy or laminotomy with fusion. Patients undergoing decompression with fusion had higher mean mortality (estimated probability 0.0034 vs. 0.0027, p<0.001), mean morbidity (estimated probability 0.053 vs. 0.048, p<0.001), mean length of stay (3.62±3.4 days vs. 3.15±4.3 days, p<0.001), and bleeding risk necessitating transfusion (9.5% vs. 7.6%, p =0.038). There was a higher rate of overall 30-day postoperative complications associated with an increasing ASA score for both cohorts.
Conclusions: Decompression with fusion was associated with higher estimated mortality, morbidity, and 30-day complications. Decompression alone is an appealing treatment option for lumbar DS, particularly for patients with higher ASA scores and those at higher risk.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


