Senta Frol, Faysal Benali, Aymeric Rouchaud, Robrecht R M M Knapen, Wim H van Zwam
{"title":"在血管内卒中治疗期间,肝素通过静脉注射和冲洗液系统的不同使用,一项世界性的调查。","authors":"Senta Frol, Faysal Benali, Aymeric Rouchaud, Robrecht R M M Knapen, Wim H van Zwam","doi":"10.1186/s42155-025-00532-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The total amount of heparin administered through flush fluids in stroke patients is not considered in recent trials, possibly influencing main results. We investigated the use of heparin among treating physicians worldwide.</p><p><strong>Methods: </strong>We conducted a survey from November 2022 to January 2023 to identify the variability of heparin administration during stroke endovascular treatment (EVT). We calculated the total heparin dose per hour (IU/h) by adding the intravenous (IV)-bolus dose to the amount administered through flush fluids, calculated by a multiplication of the number of infusion bags, drip rate[mL/h] and heparin concentration[IU/L].</p><p><strong>Results: </strong>A total of 315 participants from different countries worldwide completed the survey and 231/315(73%) respondents administer heparin during EVT. The majority administered heparin only through flush fluids (168/231; 72.7%), followed by both IV-bolus and flush fluids (36/231; 16%), and those who used only an IV-bolus (27/231; 11.7%). From the participants that administer heparin through flush fluids, the median heparin concentration was 2000 IU/L (range:100 IU/L-10000 IU/L). The total heparin dose (administered through flush fluids and IV-bolus) among 23 respondents showed a median of 4650 IU/h (IQR:3432-5900). Among the respondents who administer heparin through IV-bolus only, the median was 5250 IU (IQR:3750-7500).</p><p><strong>Conclusion: </strong>This survey revealed variable heparin doses administered by physicians worldwide during EVT and reflects the lack of international guidelines. Caution is warranted, specifically during complex/long EVT procedures. Furthermore, heparin flush doses should be considered in future trials regarding periprocedural anticoagulants, since imbalances could potentially confound results.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"8 1","pages":"17"},"PeriodicalIF":1.5000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11872961/pdf/","citationCount":"0","resultStr":"{\"title\":\"The variable use of heparin through intravenous bolus and flush fluid systems during endovascular stroke treatment, a world-wide survey.\",\"authors\":\"Senta Frol, Faysal Benali, Aymeric Rouchaud, Robrecht R M M Knapen, Wim H van Zwam\",\"doi\":\"10.1186/s42155-025-00532-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The total amount of heparin administered through flush fluids in stroke patients is not considered in recent trials, possibly influencing main results. We investigated the use of heparin among treating physicians worldwide.</p><p><strong>Methods: </strong>We conducted a survey from November 2022 to January 2023 to identify the variability of heparin administration during stroke endovascular treatment (EVT). We calculated the total heparin dose per hour (IU/h) by adding the intravenous (IV)-bolus dose to the amount administered through flush fluids, calculated by a multiplication of the number of infusion bags, drip rate[mL/h] and heparin concentration[IU/L].</p><p><strong>Results: </strong>A total of 315 participants from different countries worldwide completed the survey and 231/315(73%) respondents administer heparin during EVT. The majority administered heparin only through flush fluids (168/231; 72.7%), followed by both IV-bolus and flush fluids (36/231; 16%), and those who used only an IV-bolus (27/231; 11.7%). From the participants that administer heparin through flush fluids, the median heparin concentration was 2000 IU/L (range:100 IU/L-10000 IU/L). The total heparin dose (administered through flush fluids and IV-bolus) among 23 respondents showed a median of 4650 IU/h (IQR:3432-5900). Among the respondents who administer heparin through IV-bolus only, the median was 5250 IU (IQR:3750-7500).</p><p><strong>Conclusion: </strong>This survey revealed variable heparin doses administered by physicians worldwide during EVT and reflects the lack of international guidelines. Caution is warranted, specifically during complex/long EVT procedures. Furthermore, heparin flush doses should be considered in future trials regarding periprocedural anticoagulants, since imbalances could potentially confound results.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":\"8 1\",\"pages\":\"17\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-03-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11872961/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-025-00532-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-025-00532-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:最近的试验未考虑脑卒中患者通过冲洗液给予肝素的总量,这可能影响主要结果。我们调查了世界范围内治疗医生使用肝素的情况。方法:我们于2022年11月至2023年1月进行了一项调查,以确定脑卒中血管内治疗(EVT)期间肝素给药的变异性。我们通过将静脉(IV)丸剂量与冲洗液给药量相加,计算出每小时肝素总剂量(IU/h),计算方法是将输液袋数、滴注速率[mL/h]和肝素浓度[IU/L]相乘。结果:来自全球不同国家的315名参与者完成了调查,231/315(73%)的受访者在EVT期间使用肝素。大多数患者仅通过冲洗液给予肝素(168/231;72.7%),其次是静脉注射和冲洗液(36/231;16%),以及仅使用静脉注射的患者(27/231;11.7%)。通过冲洗液给予肝素的参与者,肝素浓度中位数为2000 IU/L(范围:100 IU/L-10000 IU/L)。23名应答者的总肝素剂量(通过冲洗液和静脉注射)中位数为4650 IU/h (IQR:3432-5900)。在仅通过静脉注射给药肝素的应答者中,中位数为5250 IU (IQR:3750-7500)。结论:这项调查揭示了世界各地的医生在EVT期间使用不同的肝素剂量,反映了缺乏国际指南。谨慎是必要的,特别是在复杂/漫长的EVT过程中。此外,在未来的围手术期抗凝剂试验中应考虑肝素冲洗剂量,因为不平衡可能会混淆结果。
The variable use of heparin through intravenous bolus and flush fluid systems during endovascular stroke treatment, a world-wide survey.
Background: The total amount of heparin administered through flush fluids in stroke patients is not considered in recent trials, possibly influencing main results. We investigated the use of heparin among treating physicians worldwide.
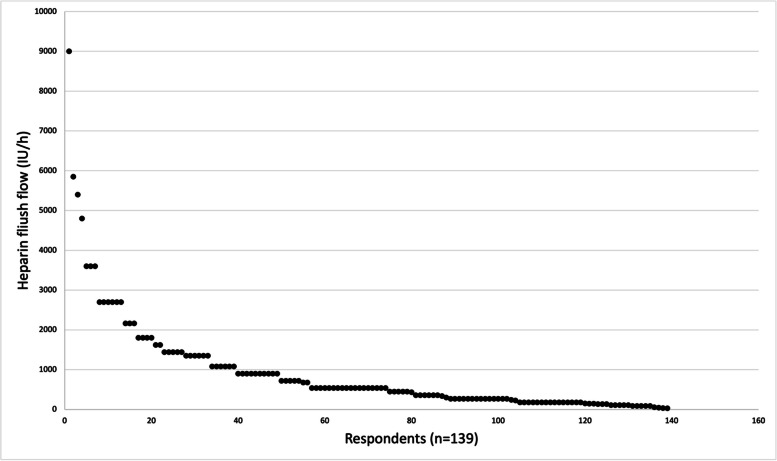
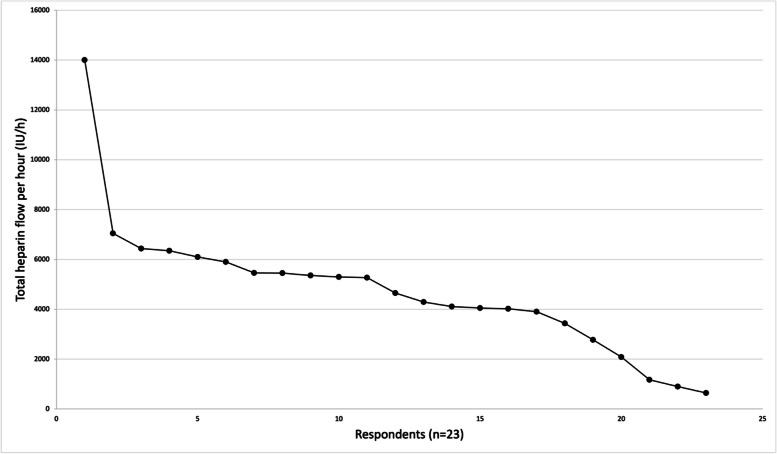
Methods: We conducted a survey from November 2022 to January 2023 to identify the variability of heparin administration during stroke endovascular treatment (EVT). We calculated the total heparin dose per hour (IU/h) by adding the intravenous (IV)-bolus dose to the amount administered through flush fluids, calculated by a multiplication of the number of infusion bags, drip rate[mL/h] and heparin concentration[IU/L].
Results: A total of 315 participants from different countries worldwide completed the survey and 231/315(73%) respondents administer heparin during EVT. The majority administered heparin only through flush fluids (168/231; 72.7%), followed by both IV-bolus and flush fluids (36/231; 16%), and those who used only an IV-bolus (27/231; 11.7%). From the participants that administer heparin through flush fluids, the median heparin concentration was 2000 IU/L (range:100 IU/L-10000 IU/L). The total heparin dose (administered through flush fluids and IV-bolus) among 23 respondents showed a median of 4650 IU/h (IQR:3432-5900). Among the respondents who administer heparin through IV-bolus only, the median was 5250 IU (IQR:3750-7500).
Conclusion: This survey revealed variable heparin doses administered by physicians worldwide during EVT and reflects the lack of international guidelines. Caution is warranted, specifically during complex/long EVT procedures. Furthermore, heparin flush doses should be considered in future trials regarding periprocedural anticoagulants, since imbalances could potentially confound results.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


