Alexandre Descamps, Matthias Jacquet-Lagrèze, Thomas Aussal, Jean-Luc Fellahi, Martin Ruste
{"title":"DiCARTTM装置测量毛细血管再充血时间:急性循环衰竭患者的验证研究。","authors":"Alexandre Descamps, Matthias Jacquet-Lagrèze, Thomas Aussal, Jean-Luc Fellahi, Martin Ruste","doi":"10.1007/s10877-025-01271-5","DOIUrl":null,"url":null,"abstract":"<p><p>Capillary Refill Time (CRT) is a valuable metric to assess cutaneous perfusion. Its prognostic value in patients with acute circulatory failure has been reported as improved when the measurement is standardized. The DiCART™ device is a fully automated CRT measurement tool requiring validation. We conducted a comparative interventional single-center study including 25 patients with acute circulatory failure, to evaluate the agreement between CRT measured by an automated measurement device (CRT<sub>DiCART</sub>) and CRT measured clinically (CRT<sub>CLIN</sub>). CRT was measured on the fingertip, chest, and knee. Three measurements were performed at each location to obtain an average for each site. The measurements were conducted both clinically and using the DiCART™ device by two different operators, each blinded to the results. Agreement was determined using intraclass correlation coefficient (ICC) and Bland and Altman analysis. The ICC between CRT<sub>CLIN</sub> and CRT<sub>DiCART</sub> was 0.46 (95% Confidence Interval (CI) 0.32, 0.59) across all measurement sites; the mean bias was 0.23s (95% CI -0.17, 0.64), with upper Limit of Agreement (LoA) 2.77s (95% CI 2.44, 3.20) and lower LoA - 2.30s (-2.73, -1.97). Intra observer ICC was 0.85 (95% CI 0.74, 0.91) for CRT<sub>CLIN</sub> and 0.43 (95% CI 0.15, 0.64) for CRT<sub>DICART</sub>. Inter observer ICC was 0.86 (95% CI 0.76, 0.92) for CRT<sub>CLIN</sub> and was 0.41 (95% CI 0.14, 0,63) for CRT<sub>DICART</sub>. The DiCART™ device showed poor agreement with clinical CRT in patients with acute circulatory failure, which does not support its use in routine practice.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"831-840"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474624/pdf/","citationCount":"0","resultStr":"{\"title\":\"DiCART<sup>TM</sup> device to measure capillary refill time: a validation study in patients with acute circulatory failure.\",\"authors\":\"Alexandre Descamps, Matthias Jacquet-Lagrèze, Thomas Aussal, Jean-Luc Fellahi, Martin Ruste\",\"doi\":\"10.1007/s10877-025-01271-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Capillary Refill Time (CRT) is a valuable metric to assess cutaneous perfusion. Its prognostic value in patients with acute circulatory failure has been reported as improved when the measurement is standardized. The DiCART™ device is a fully automated CRT measurement tool requiring validation. We conducted a comparative interventional single-center study including 25 patients with acute circulatory failure, to evaluate the agreement between CRT measured by an automated measurement device (CRT<sub>DiCART</sub>) and CRT measured clinically (CRT<sub>CLIN</sub>). CRT was measured on the fingertip, chest, and knee. Three measurements were performed at each location to obtain an average for each site. The measurements were conducted both clinically and using the DiCART™ device by two different operators, each blinded to the results. Agreement was determined using intraclass correlation coefficient (ICC) and Bland and Altman analysis. The ICC between CRT<sub>CLIN</sub> and CRT<sub>DiCART</sub> was 0.46 (95% Confidence Interval (CI) 0.32, 0.59) across all measurement sites; the mean bias was 0.23s (95% CI -0.17, 0.64), with upper Limit of Agreement (LoA) 2.77s (95% CI 2.44, 3.20) and lower LoA - 2.30s (-2.73, -1.97). Intra observer ICC was 0.85 (95% CI 0.74, 0.91) for CRT<sub>CLIN</sub> and 0.43 (95% CI 0.15, 0.64) for CRT<sub>DICART</sub>. Inter observer ICC was 0.86 (95% CI 0.76, 0.92) for CRT<sub>CLIN</sub> and was 0.41 (95% CI 0.14, 0,63) for CRT<sub>DICART</sub>. The DiCART™ device showed poor agreement with clinical CRT in patients with acute circulatory failure, which does not support its use in routine practice.</p>\",\"PeriodicalId\":15513,\"journal\":{\"name\":\"Journal of Clinical Monitoring and Computing\",\"volume\":\" \",\"pages\":\"831-840\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474624/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Monitoring and Computing\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10877-025-01271-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-025-01271-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/26 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
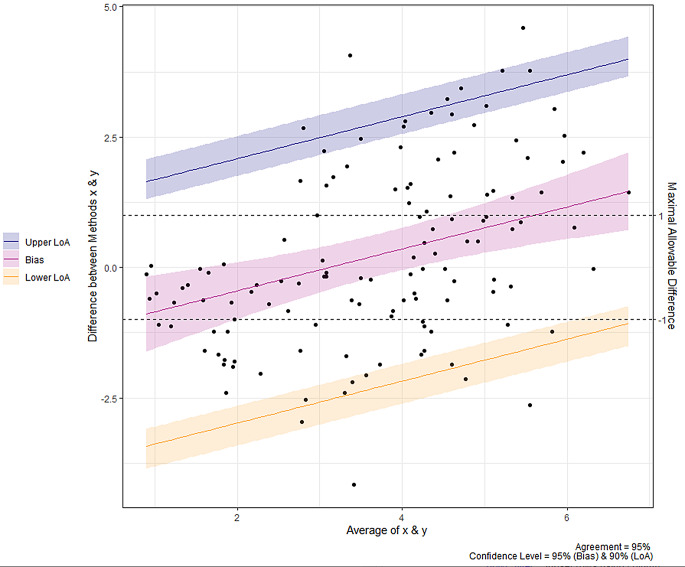
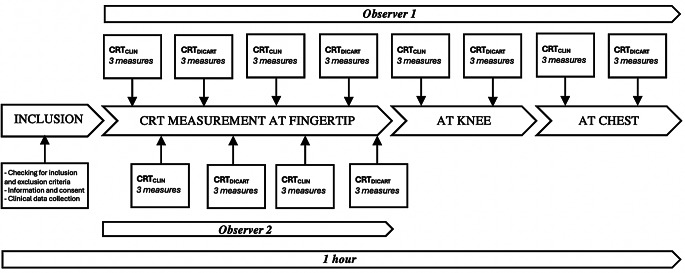
毛细管再充血时间(CRT)是评估皮肤灌注的重要指标。据报道,当测量标准化后,其对急性循环衰竭患者的预后价值有所提高。DiCART™设备是一种需要验证的全自动CRT测量工具。我们进行了一项比较介入单中心研究,包括25例急性循环衰竭患者,以评估自动测量装置(CRTDiCART)测量的CRT与临床测量的CRT (CRTCLIN)之间的一致性。在指尖、胸部和膝盖处测量CRT。在每个地点进行了三次测量,以获得每个地点的平均值。测量由两名不同的操作人员在临床上和使用DiCART™设备进行,每名操作人员对结果都不知情。采用类内相关系数(ICC)和Bland和Altman分析来确定一致性。在所有测量点,CRTCLIN和CRTDiCART之间的ICC为0.46(95%置信区间(CI) 0.32, 0.59);平均偏差为0.23s (95% CI -0.17, 0.64),一致性上限(LoA)为2.77s (95% CI 2.44, 3.20),下限为2.30s(-2.73, -1.97)。CRTCLIN的观察者内ICC为0.85 (95% CI 0.74, 0.91), CRTDICART的观察者内ICC为0.43 (95% CI 0.15, 0.64)。CRTCLIN的观察者间ICC为0.86 (95% CI 0.76, 0.92), CRTDICART的观察者间ICC为0.41 (95% CI 0.14, 0,63)。在急性循环衰竭患者中,DiCART™装置与临床CRT的一致性较差,因此不支持其在常规实践中使用。
DiCARTTM device to measure capillary refill time: a validation study in patients with acute circulatory failure.
Capillary Refill Time (CRT) is a valuable metric to assess cutaneous perfusion. Its prognostic value in patients with acute circulatory failure has been reported as improved when the measurement is standardized. The DiCART™ device is a fully automated CRT measurement tool requiring validation. We conducted a comparative interventional single-center study including 25 patients with acute circulatory failure, to evaluate the agreement between CRT measured by an automated measurement device (CRTDiCART) and CRT measured clinically (CRTCLIN). CRT was measured on the fingertip, chest, and knee. Three measurements were performed at each location to obtain an average for each site. The measurements were conducted both clinically and using the DiCART™ device by two different operators, each blinded to the results. Agreement was determined using intraclass correlation coefficient (ICC) and Bland and Altman analysis. The ICC between CRTCLIN and CRTDiCART was 0.46 (95% Confidence Interval (CI) 0.32, 0.59) across all measurement sites; the mean bias was 0.23s (95% CI -0.17, 0.64), with upper Limit of Agreement (LoA) 2.77s (95% CI 2.44, 3.20) and lower LoA - 2.30s (-2.73, -1.97). Intra observer ICC was 0.85 (95% CI 0.74, 0.91) for CRTCLIN and 0.43 (95% CI 0.15, 0.64) for CRTDICART. Inter observer ICC was 0.86 (95% CI 0.76, 0.92) for CRTCLIN and was 0.41 (95% CI 0.14, 0,63) for CRTDICART. The DiCART™ device showed poor agreement with clinical CRT in patients with acute circulatory failure, which does not support its use in routine practice.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


