Renuka Tolani, Steffi Sathiyaraj, David Lyu, Luan Truong, Theresa Thurston, Ziad M El-Zaatari, Ali R Khan, Angelina Edwards, Shane A Bobart
{"title":"地下室的双重麻烦!pla2r相关性膜性肾病合并非典型抗肾小球基底膜病1例。","authors":"Renuka Tolani, Steffi Sathiyaraj, David Lyu, Luan Truong, Theresa Thurston, Ziad M El-Zaatari, Ali R Khan, Angelina Edwards, Shane A Bobart","doi":"10.1159/000542859","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Concurrent atypical anti-glomerular basement membrane (anti-GBM) disease with membranous nephropathy is a rare occurrence. Compared to typical anti-GBM disease, atypical anti-GBM disease is often seronegative, with a mild disease presentation and course. We present a case of concomitant of PLA2R-associated membranous nephropathy and atypical anti-GBM disease in a patient with cholangiocarcinoma.</p><p><strong>Case presentation: </strong>A 66-year-old male with type 2 diabetes, hypertension, hyperlipidemia, hepatitis C, cirrhosis, and cholangiocarcinoma presented with nephrotic range proteinuria and worsening bilateral lower extremity edema. Urine studies showed 3+ protein and 13 red blood cells per high power field and 24-h urine protein of 14 g (nephrotic range). Serum albumin was 2.1 g/dL and serum creatinine was 0.8 mg/dL (nephrotic syndrome). Serological work-up was negative for antinuclear antibody, anti-double stranded DNA antibody, anti-PLA2R, anti-neutrophil cytoplasmic antibody, rheumatoid factor, and anti-GBM. Complement (C3 and C4) levels were normal and no monoclonal gammopathy was detected. A kidney biopsy showed membranous nephropathy with typical light microscopic, immunofluorescence, and electron microscopic findings. In addition, there was atypical anti-GBM disease characterized by a non-circumferential cellular crescent in 1 out of 12 glomeruli 2-3+ linear staining for IgG along GBM. There was no tubular basement membrane staining for IgG and albumin staining was negative. The glomeruli demonstrated strong staining for PLA2R but were negative for THSD7A and NELL-1. The patient received rituximab infusion, dapagliflozin, and lisinopril, resulting in remission of proteinuria. Despite intense chemotherapy with cisplatin, gemcitabine, and immunotherapy, the patient's cholangiocarcinoma progressed, and he transitioned to hospice care.</p><p><strong>Conclusion: </strong>For our patient, rituximab resulted in remission of proteinuria. The lack of temporal association with the malignancy is consistent with the biopsy findings of PLA2R-associated membranous nephropathy. While there is not an established guideline for atypical anti-GBM disease, our case demonstrates the utility of rituximab for the management of concurrent atypical anti-GBM disease with membranous nephropathy.</p>","PeriodicalId":73177,"journal":{"name":"Glomerular diseases","volume":"5 1","pages":"13-18"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842034/pdf/","citationCount":"0","resultStr":"{\"title\":\"Double Trouble in the Basement! A Case of PLA2R-Associated Membranous Nephropathy with Atypical Anti-Glomerular Basement Membrane Disease.\",\"authors\":\"Renuka Tolani, Steffi Sathiyaraj, David Lyu, Luan Truong, Theresa Thurston, Ziad M El-Zaatari, Ali R Khan, Angelina Edwards, Shane A Bobart\",\"doi\":\"10.1159/000542859\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Concurrent atypical anti-glomerular basement membrane (anti-GBM) disease with membranous nephropathy is a rare occurrence. Compared to typical anti-GBM disease, atypical anti-GBM disease is often seronegative, with a mild disease presentation and course. We present a case of concomitant of PLA2R-associated membranous nephropathy and atypical anti-GBM disease in a patient with cholangiocarcinoma.</p><p><strong>Case presentation: </strong>A 66-year-old male with type 2 diabetes, hypertension, hyperlipidemia, hepatitis C, cirrhosis, and cholangiocarcinoma presented with nephrotic range proteinuria and worsening bilateral lower extremity edema. Urine studies showed 3+ protein and 13 red blood cells per high power field and 24-h urine protein of 14 g (nephrotic range). Serum albumin was 2.1 g/dL and serum creatinine was 0.8 mg/dL (nephrotic syndrome). Serological work-up was negative for antinuclear antibody, anti-double stranded DNA antibody, anti-PLA2R, anti-neutrophil cytoplasmic antibody, rheumatoid factor, and anti-GBM. Complement (C3 and C4) levels were normal and no monoclonal gammopathy was detected. A kidney biopsy showed membranous nephropathy with typical light microscopic, immunofluorescence, and electron microscopic findings. In addition, there was atypical anti-GBM disease characterized by a non-circumferential cellular crescent in 1 out of 12 glomeruli 2-3+ linear staining for IgG along GBM. There was no tubular basement membrane staining for IgG and albumin staining was negative. The glomeruli demonstrated strong staining for PLA2R but were negative for THSD7A and NELL-1. The patient received rituximab infusion, dapagliflozin, and lisinopril, resulting in remission of proteinuria. Despite intense chemotherapy with cisplatin, gemcitabine, and immunotherapy, the patient's cholangiocarcinoma progressed, and he transitioned to hospice care.</p><p><strong>Conclusion: </strong>For our patient, rituximab resulted in remission of proteinuria. The lack of temporal association with the malignancy is consistent with the biopsy findings of PLA2R-associated membranous nephropathy. While there is not an established guideline for atypical anti-GBM disease, our case demonstrates the utility of rituximab for the management of concurrent atypical anti-GBM disease with membranous nephropathy.</p>\",\"PeriodicalId\":73177,\"journal\":{\"name\":\"Glomerular diseases\",\"volume\":\"5 1\",\"pages\":\"13-18\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11842034/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Glomerular diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000542859\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Glomerular diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000542859","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Double Trouble in the Basement! A Case of PLA2R-Associated Membranous Nephropathy with Atypical Anti-Glomerular Basement Membrane Disease.
Introduction: Concurrent atypical anti-glomerular basement membrane (anti-GBM) disease with membranous nephropathy is a rare occurrence. Compared to typical anti-GBM disease, atypical anti-GBM disease is often seronegative, with a mild disease presentation and course. We present a case of concomitant of PLA2R-associated membranous nephropathy and atypical anti-GBM disease in a patient with cholangiocarcinoma.
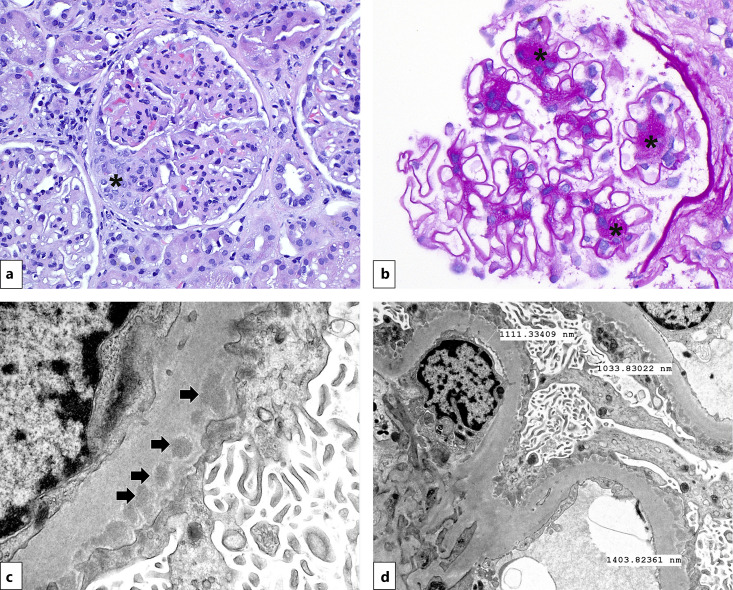
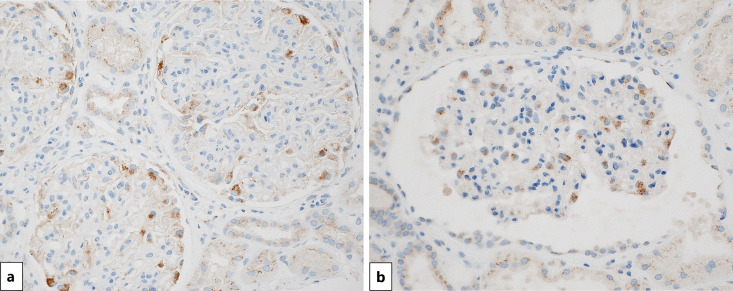
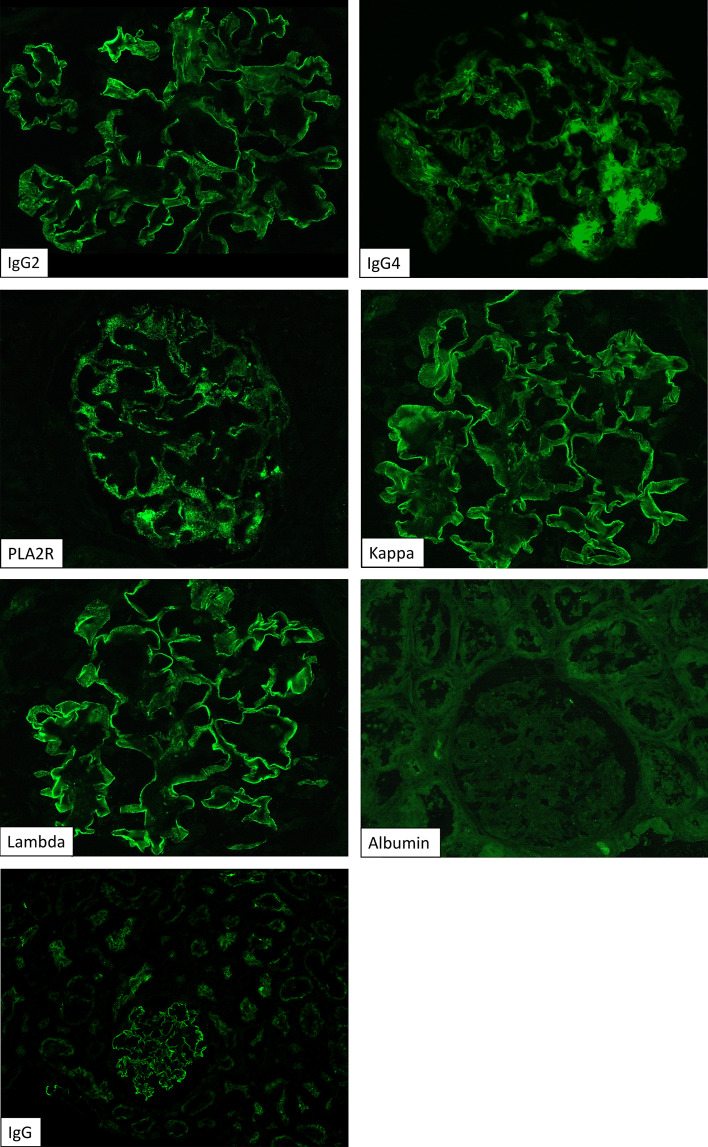
Case presentation: A 66-year-old male with type 2 diabetes, hypertension, hyperlipidemia, hepatitis C, cirrhosis, and cholangiocarcinoma presented with nephrotic range proteinuria and worsening bilateral lower extremity edema. Urine studies showed 3+ protein and 13 red blood cells per high power field and 24-h urine protein of 14 g (nephrotic range). Serum albumin was 2.1 g/dL and serum creatinine was 0.8 mg/dL (nephrotic syndrome). Serological work-up was negative for antinuclear antibody, anti-double stranded DNA antibody, anti-PLA2R, anti-neutrophil cytoplasmic antibody, rheumatoid factor, and anti-GBM. Complement (C3 and C4) levels were normal and no monoclonal gammopathy was detected. A kidney biopsy showed membranous nephropathy with typical light microscopic, immunofluorescence, and electron microscopic findings. In addition, there was atypical anti-GBM disease characterized by a non-circumferential cellular crescent in 1 out of 12 glomeruli 2-3+ linear staining for IgG along GBM. There was no tubular basement membrane staining for IgG and albumin staining was negative. The glomeruli demonstrated strong staining for PLA2R but were negative for THSD7A and NELL-1. The patient received rituximab infusion, dapagliflozin, and lisinopril, resulting in remission of proteinuria. Despite intense chemotherapy with cisplatin, gemcitabine, and immunotherapy, the patient's cholangiocarcinoma progressed, and he transitioned to hospice care.
Conclusion: For our patient, rituximab resulted in remission of proteinuria. The lack of temporal association with the malignancy is consistent with the biopsy findings of PLA2R-associated membranous nephropathy. While there is not an established guideline for atypical anti-GBM disease, our case demonstrates the utility of rituximab for the management of concurrent atypical anti-GBM disease with membranous nephropathy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


