Ria Nagpal, Marina Campione, Sara Elena Rebuzzi, Lucia Fratino, Pasquale Rescigno, Sergio Bracarda, Davide Bimbatti, Ugo De Giorgi, Matteo Santoni, Fabio Calabrò, Mimma Rizzo, Alessio Signori, Diana Giannarelli, Giuseppe Fornarini, Umberto Basso, Giuseppe Luigi Banna
{"title":"G8老年筛查和met - uro评分在接受伊匹单抗-纳沃单抗一线联合免疫治疗的转移性肾癌患者中的预后价值","authors":"Ria Nagpal, Marina Campione, Sara Elena Rebuzzi, Lucia Fratino, Pasquale Rescigno, Sergio Bracarda, Davide Bimbatti, Ugo De Giorgi, Matteo Santoni, Fabio Calabrò, Mimma Rizzo, Alessio Signori, Diana Giannarelli, Giuseppe Fornarini, Umberto Basso, Giuseppe Luigi Banna","doi":"10.1177/15330338251316626","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The prognostic value of the Geriatric 8 (G8) screening score in metastatic renal cell carcinoma (mRCC) patients receiving first-line immunotherapy remains unclear. This study aimed to evaluate the prognostic role of G8 within the context of the Meet-URO classification in mRCC patients treated with first-line ipilimumab-nivolumab.</p><p><strong>Methods: </strong>This retrospective multicentre study analysed 106 mRCC patients treated with first-line ipilimumab-nivolumab. G8 and Meet-URO scores were calculated before treatment initiation. Primary endpoint was overall survival (OS), defined as duration from first administration of Nivolumab to death. OS was analysed in relation to age groups, G8 scores, and Meet-URO score categories, with data censored for patients still alive at the last follow-up. The secondary endpoint, progression-free survival (PFS), was measured from initiating Nivolumab to the earliest instance of disease progression or death. OS and PFS were assessed using Kaplan-Meier methods and Cox regression analyses. The reporting of this study conforms to the REMARK guidelines.</p><p><strong>Results: </strong>Patients with G8 > 14 had more favorable IMDC and Meet-URO risk classifications and lower neutrophil-to-lymphocyte ratios. While PFS did not differ significantly between G8 ≤ 14 and >14 groups (1-year 29.3% vs 46.2%, p = 0.2), OS was significantly longer in G8 > 14 group (1-year 76.1% vs 58.6%, p = 0.006). In multivariable analysis, G8 ≤ 14 was independently associated with worse OS (HR 2.36, 95% CI 1.06-5.08, p = 0.03) but not PFS. The Meet-URO score was prognostic for both PFS and OS. In patients ≥70 years, G8 lost its prognostic value, while Meet-URO remained prognostic for OS.</p><p><strong>Conclusions: </strong>The G8 score is an independent prognostic factor for OS but not PFS in mRCC patients receiving first-line ipilimumab-nivolumab. The Meet-URO score shows consistent prognostic ability for PFS and OS across age groups. These findings suggest that while G8 may be useful for individual patient-level OS prediction, the Meet-URO score may be superior for guiding treatment decisions in clinical practice.</p>","PeriodicalId":22203,"journal":{"name":"Technology in Cancer Research & Treatment","volume":"24 ","pages":"15330338251316626"},"PeriodicalIF":2.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11848895/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic Value of G8 Geriatric Screening and Meet-URO Scores in Metastatic Renal Cell Carcinoma Patients Receiving First-Line Ipilimumab-Nivolumab Combination Immunotherapy.\",\"authors\":\"Ria Nagpal, Marina Campione, Sara Elena Rebuzzi, Lucia Fratino, Pasquale Rescigno, Sergio Bracarda, Davide Bimbatti, Ugo De Giorgi, Matteo Santoni, Fabio Calabrò, Mimma Rizzo, Alessio Signori, Diana Giannarelli, Giuseppe Fornarini, Umberto Basso, Giuseppe Luigi Banna\",\"doi\":\"10.1177/15330338251316626\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The prognostic value of the Geriatric 8 (G8) screening score in metastatic renal cell carcinoma (mRCC) patients receiving first-line immunotherapy remains unclear. This study aimed to evaluate the prognostic role of G8 within the context of the Meet-URO classification in mRCC patients treated with first-line ipilimumab-nivolumab.</p><p><strong>Methods: </strong>This retrospective multicentre study analysed 106 mRCC patients treated with first-line ipilimumab-nivolumab. G8 and Meet-URO scores were calculated before treatment initiation. Primary endpoint was overall survival (OS), defined as duration from first administration of Nivolumab to death. OS was analysed in relation to age groups, G8 scores, and Meet-URO score categories, with data censored for patients still alive at the last follow-up. The secondary endpoint, progression-free survival (PFS), was measured from initiating Nivolumab to the earliest instance of disease progression or death. OS and PFS were assessed using Kaplan-Meier methods and Cox regression analyses. The reporting of this study conforms to the REMARK guidelines.</p><p><strong>Results: </strong>Patients with G8 > 14 had more favorable IMDC and Meet-URO risk classifications and lower neutrophil-to-lymphocyte ratios. While PFS did not differ significantly between G8 ≤ 14 and >14 groups (1-year 29.3% vs 46.2%, p = 0.2), OS was significantly longer in G8 > 14 group (1-year 76.1% vs 58.6%, p = 0.006). In multivariable analysis, G8 ≤ 14 was independently associated with worse OS (HR 2.36, 95% CI 1.06-5.08, p = 0.03) but not PFS. The Meet-URO score was prognostic for both PFS and OS. In patients ≥70 years, G8 lost its prognostic value, while Meet-URO remained prognostic for OS.</p><p><strong>Conclusions: </strong>The G8 score is an independent prognostic factor for OS but not PFS in mRCC patients receiving first-line ipilimumab-nivolumab. The Meet-URO score shows consistent prognostic ability for PFS and OS across age groups. These findings suggest that while G8 may be useful for individual patient-level OS prediction, the Meet-URO score may be superior for guiding treatment decisions in clinical practice.</p>\",\"PeriodicalId\":22203,\"journal\":{\"name\":\"Technology in Cancer Research & Treatment\",\"volume\":\"24 \",\"pages\":\"15330338251316626\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11848895/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Technology in Cancer Research & Treatment\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/15330338251316626\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Technology in Cancer Research & Treatment","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15330338251316626","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:老年8 (G8)筛查评分在接受一线免疫治疗的转移性肾细胞癌(mRCC)患者中的预后价值尚不清楚。本研究旨在评估G8在met - uro分类背景下对一线伊匹单抗-纳武单抗治疗的mRCC患者的预后作用。方法:这项回顾性多中心研究分析了106例一线伊匹单抗-纳武单抗治疗的mRCC患者。在治疗开始前计算G8和met - uro评分。主要终点是总生存期(OS),定义为从第一次给药到死亡的持续时间。分析OS与年龄组、G8评分和Meet-URO评分类别的关系,对最后一次随访时仍然存活的患者进行数据删除。次要终点,无进展生存期(PFS),从开始Nivolumab到最早的疾病进展或死亡实例进行测量。采用Kaplan-Meier法和Cox回归分析评价OS和PFS。本研究的报告符合REMARK指南。结果:G8 bbb14患者IMDC和met - uro风险分级更有利,中性粒细胞与淋巴细胞比值更低。虽然G8≤14组和>4组的PFS无显著差异(1年29.3% vs 46.2%, p = 0.2),但G8≤14组的OS明显更长(1年76.1% vs 58.6%, p = 0.006)。在多变量分析中,G8≤14与较差的OS独立相关(HR 2.36, 95% CI 1.06 ~ 5.08, p = 0.03),但与PFS无关。met - uro评分是PFS和OS的预后指标。在≥70岁的患者中,G8失去了预后价值,而met - uro仍然是OS的预后价值。结论:G8评分是接受一线伊匹单抗-纳沃单抗治疗的mRCC患者OS的独立预后因素,而不是PFS。Meet-URO评分显示各年龄组PFS和OS的预后能力一致。这些发现表明,虽然G8可能对个体患者水平的OS预测有用,但met - uro评分可能在指导临床实践中的治疗决策方面更优越。
Prognostic Value of G8 Geriatric Screening and Meet-URO Scores in Metastatic Renal Cell Carcinoma Patients Receiving First-Line Ipilimumab-Nivolumab Combination Immunotherapy.
Background: The prognostic value of the Geriatric 8 (G8) screening score in metastatic renal cell carcinoma (mRCC) patients receiving first-line immunotherapy remains unclear. This study aimed to evaluate the prognostic role of G8 within the context of the Meet-URO classification in mRCC patients treated with first-line ipilimumab-nivolumab.
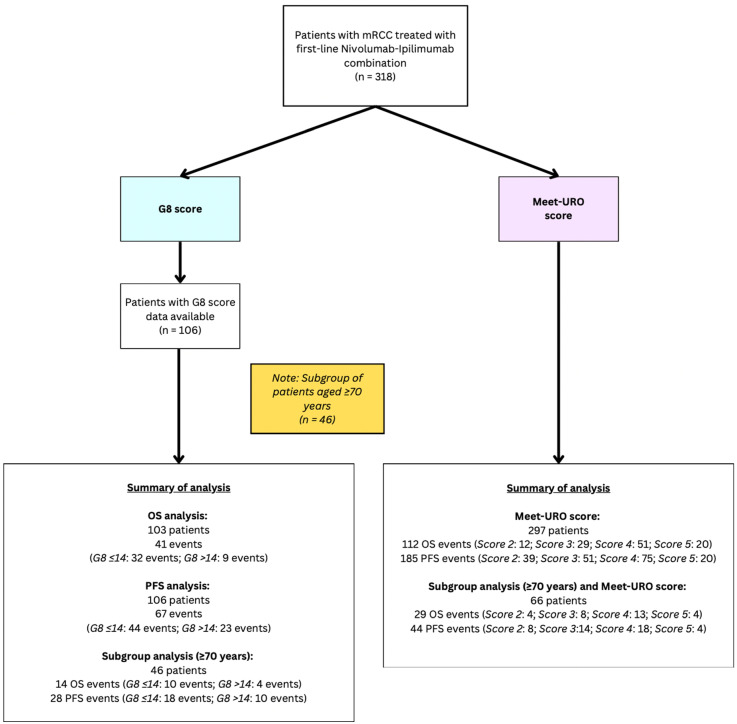
Methods: This retrospective multicentre study analysed 106 mRCC patients treated with first-line ipilimumab-nivolumab. G8 and Meet-URO scores were calculated before treatment initiation. Primary endpoint was overall survival (OS), defined as duration from first administration of Nivolumab to death. OS was analysed in relation to age groups, G8 scores, and Meet-URO score categories, with data censored for patients still alive at the last follow-up. The secondary endpoint, progression-free survival (PFS), was measured from initiating Nivolumab to the earliest instance of disease progression or death. OS and PFS were assessed using Kaplan-Meier methods and Cox regression analyses. The reporting of this study conforms to the REMARK guidelines.
Results: Patients with G8 > 14 had more favorable IMDC and Meet-URO risk classifications and lower neutrophil-to-lymphocyte ratios. While PFS did not differ significantly between G8 ≤ 14 and >14 groups (1-year 29.3% vs 46.2%, p = 0.2), OS was significantly longer in G8 > 14 group (1-year 76.1% vs 58.6%, p = 0.006). In multivariable analysis, G8 ≤ 14 was independently associated with worse OS (HR 2.36, 95% CI 1.06-5.08, p = 0.03) but not PFS. The Meet-URO score was prognostic for both PFS and OS. In patients ≥70 years, G8 lost its prognostic value, while Meet-URO remained prognostic for OS.
Conclusions: The G8 score is an independent prognostic factor for OS but not PFS in mRCC patients receiving first-line ipilimumab-nivolumab. The Meet-URO score shows consistent prognostic ability for PFS and OS across age groups. These findings suggest that while G8 may be useful for individual patient-level OS prediction, the Meet-URO score may be superior for guiding treatment decisions in clinical practice.
期刊介绍:
Technology in Cancer Research & Treatment (TCRT) is a JCR-ranked, broad-spectrum, open access, peer-reviewed publication whose aim is to provide researchers and clinicians with a platform to share and discuss developments in the prevention, diagnosis, treatment, and monitoring of cancer.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


