{"title":"以磁共振质子密度脂肪分数为参考标准的衰减成像与控制衰减参数对肝脂肪变性的诊断价值:一项前瞻性多中心研究。","authors":"Takashi Nishimura, Toshifumi Tada, Tomoyuki Akita, Reiichiro Kondo, Yasuaki Suzuki, Kento Imajo, Shigehiro Kokubu, Tamami Abe, Hidekatsu Kuroda, Masashi Hirooka, Yoichi Hiasa, Asako Nogami, Atsushi Nakajima, Sadanobu Ogawa, Hidenori Toyoda, Satoshi Oeda, Hirokazu Takahashi, Yuichiro Eguchi, Katsutoshi Sugimoto, Hirohisa Yano, Junko Tanaka, Fuminori Moriyasu, Masayoshi Kage, Takashi Kumada, Hiroko Iijima","doi":"10.1007/s00535-025-02224-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Attenuation Imaging (ATI) and controlled attenuation parameter (CAP) are non-invasive ultrasound-based methods for diagnosing hepatic steatosis. However, reports on the clinical usefulness of ATI are limited. We aimed to compare the ability of ATI and CAP to diagnose hepatic steatosis with magnetic resonance imaging-based proton density fat fraction (MRI-PDFF) as the reference standard.</p><p><strong>Methods: </strong>We performed a prospective multicenter study of 562 patients with chronic liver disease who underwent ATI, CAP, and MRI-PDFF. Patients with skin-to-liver capsule distance (SCD) ≤ 25 mm underwent CAP with an M probe; those with SCD > 25 mm underwent CAP with an XL probe. MRI-PDFF was used as the reference standard: S0 corresponds to MRI-PDFF < 5.2%, S1 to 5.2% ≤ MRI-PDFF < 11.3%, S2 to 11.3% ≤ MRI-PDFF < 17.1%, and S3 to MRI-PDFF ≥ 17.1%.</p><p><strong>Results: </strong>The correlation coefficients for ATI and MRI-PDFF stratified by body mass index (< 30, ≥ 30 kg/m<sup>2</sup>), SCD (< 25, ≥ 25 mm), 2-dimensional share wave elastography (< 1.8 m/s), fibrosis-4 index (≤ 2.67), albumin-bilirubin score (< - 2.60) and type IV collagen 7 s (< 5.0 ng/ml) were significantly higher than those for CAP and MRI-PDFF. Areas under the receiver operating characteristics (95% CI) for ATI and CAP were 0.895 (0.869-0.922) and 0.845 (0.809-0.881) for ≥ S1 steatosis, 0.944 (0.926-0.963) and 0.881(0.852-0.910) for ≥ S2 steatosis, and 0.928 (95% CI 0.906-0.950) and 0.860 (95% CI 0.829-0.890) for S3 steatosis. ATI had higher diagnostic performance for all hepatic steatosis grades than CAP.</p><p><strong>Conclusions: </strong>ATI is a more useful non-invasive method for diagnosing hepatic steatosis than CAP.</p>","PeriodicalId":16059,"journal":{"name":"Journal of Gastroenterology","volume":" ","pages":"727-737"},"PeriodicalIF":5.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12095409/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic performance of attenuation imaging versus controlled attenuation parameter for hepatic steatosis with MRI-based proton density fat fraction as the reference standard: a prospective multicenter study.\",\"authors\":\"Takashi Nishimura, Toshifumi Tada, Tomoyuki Akita, Reiichiro Kondo, Yasuaki Suzuki, Kento Imajo, Shigehiro Kokubu, Tamami Abe, Hidekatsu Kuroda, Masashi Hirooka, Yoichi Hiasa, Asako Nogami, Atsushi Nakajima, Sadanobu Ogawa, Hidenori Toyoda, Satoshi Oeda, Hirokazu Takahashi, Yuichiro Eguchi, Katsutoshi Sugimoto, Hirohisa Yano, Junko Tanaka, Fuminori Moriyasu, Masayoshi Kage, Takashi Kumada, Hiroko Iijima\",\"doi\":\"10.1007/s00535-025-02224-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Attenuation Imaging (ATI) and controlled attenuation parameter (CAP) are non-invasive ultrasound-based methods for diagnosing hepatic steatosis. However, reports on the clinical usefulness of ATI are limited. We aimed to compare the ability of ATI and CAP to diagnose hepatic steatosis with magnetic resonance imaging-based proton density fat fraction (MRI-PDFF) as the reference standard.</p><p><strong>Methods: </strong>We performed a prospective multicenter study of 562 patients with chronic liver disease who underwent ATI, CAP, and MRI-PDFF. Patients with skin-to-liver capsule distance (SCD) ≤ 25 mm underwent CAP with an M probe; those with SCD > 25 mm underwent CAP with an XL probe. MRI-PDFF was used as the reference standard: S0 corresponds to MRI-PDFF < 5.2%, S1 to 5.2% ≤ MRI-PDFF < 11.3%, S2 to 11.3% ≤ MRI-PDFF < 17.1%, and S3 to MRI-PDFF ≥ 17.1%.</p><p><strong>Results: </strong>The correlation coefficients for ATI and MRI-PDFF stratified by body mass index (< 30, ≥ 30 kg/m<sup>2</sup>), SCD (< 25, ≥ 25 mm), 2-dimensional share wave elastography (< 1.8 m/s), fibrosis-4 index (≤ 2.67), albumin-bilirubin score (< - 2.60) and type IV collagen 7 s (< 5.0 ng/ml) were significantly higher than those for CAP and MRI-PDFF. Areas under the receiver operating characteristics (95% CI) for ATI and CAP were 0.895 (0.869-0.922) and 0.845 (0.809-0.881) for ≥ S1 steatosis, 0.944 (0.926-0.963) and 0.881(0.852-0.910) for ≥ S2 steatosis, and 0.928 (95% CI 0.906-0.950) and 0.860 (95% CI 0.829-0.890) for S3 steatosis. ATI had higher diagnostic performance for all hepatic steatosis grades than CAP.</p><p><strong>Conclusions: </strong>ATI is a more useful non-invasive method for diagnosing hepatic steatosis than CAP.</p>\",\"PeriodicalId\":16059,\"journal\":{\"name\":\"Journal of Gastroenterology\",\"volume\":\" \",\"pages\":\"727-737\"},\"PeriodicalIF\":5.5000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12095409/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00535-025-02224-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00535-025-02224-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/24 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Diagnostic performance of attenuation imaging versus controlled attenuation parameter for hepatic steatosis with MRI-based proton density fat fraction as the reference standard: a prospective multicenter study.
Background: Attenuation Imaging (ATI) and controlled attenuation parameter (CAP) are non-invasive ultrasound-based methods for diagnosing hepatic steatosis. However, reports on the clinical usefulness of ATI are limited. We aimed to compare the ability of ATI and CAP to diagnose hepatic steatosis with magnetic resonance imaging-based proton density fat fraction (MRI-PDFF) as the reference standard.
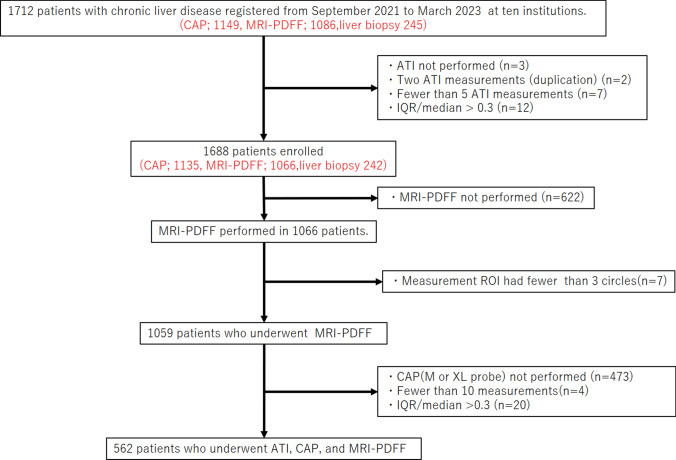
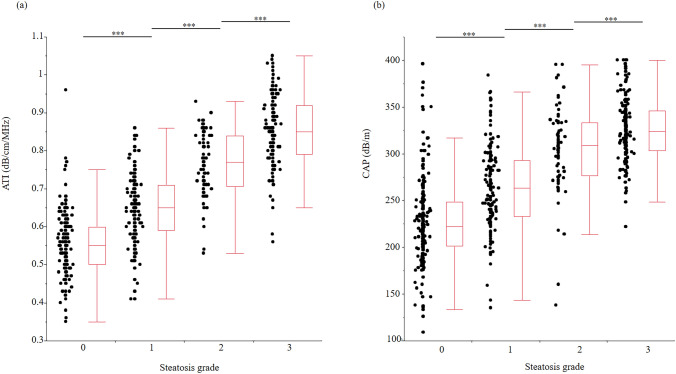
Methods: We performed a prospective multicenter study of 562 patients with chronic liver disease who underwent ATI, CAP, and MRI-PDFF. Patients with skin-to-liver capsule distance (SCD) ≤ 25 mm underwent CAP with an M probe; those with SCD > 25 mm underwent CAP with an XL probe. MRI-PDFF was used as the reference standard: S0 corresponds to MRI-PDFF < 5.2%, S1 to 5.2% ≤ MRI-PDFF < 11.3%, S2 to 11.3% ≤ MRI-PDFF < 17.1%, and S3 to MRI-PDFF ≥ 17.1%.
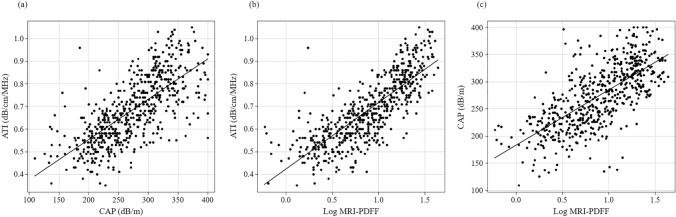
Results: The correlation coefficients for ATI and MRI-PDFF stratified by body mass index (< 30, ≥ 30 kg/m2), SCD (< 25, ≥ 25 mm), 2-dimensional share wave elastography (< 1.8 m/s), fibrosis-4 index (≤ 2.67), albumin-bilirubin score (< - 2.60) and type IV collagen 7 s (< 5.0 ng/ml) were significantly higher than those for CAP and MRI-PDFF. Areas under the receiver operating characteristics (95% CI) for ATI and CAP were 0.895 (0.869-0.922) and 0.845 (0.809-0.881) for ≥ S1 steatosis, 0.944 (0.926-0.963) and 0.881(0.852-0.910) for ≥ S2 steatosis, and 0.928 (95% CI 0.906-0.950) and 0.860 (95% CI 0.829-0.890) for S3 steatosis. ATI had higher diagnostic performance for all hepatic steatosis grades than CAP.
Conclusions: ATI is a more useful non-invasive method for diagnosing hepatic steatosis than CAP.
期刊介绍:
The Journal of Gastroenterology, which is the official publication of the Japanese Society of Gastroenterology, publishes Original Articles (Alimentary Tract/Liver, Pancreas, and Biliary Tract), Review Articles, Letters to the Editors and other articles on all aspects of the field of gastroenterology. Significant contributions relating to basic research, theory, and practice are welcomed. These publications are designed to disseminate knowledge in this field to a worldwide audience, and accordingly, its editorial board has an international membership.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


