Tingfei Tan, Siyu Yuan, Weiwei Chu, Jiemei Jiang, Meiling Chen, Quan Xia, Junping Wang
{"title":"低剂量anlotinib +免疫检查点抑制剂在晚期非小细胞肺癌治疗中具有更好的疗效和安全性。","authors":"Tingfei Tan, Siyu Yuan, Weiwei Chu, Jiemei Jiang, Meiling Chen, Quan Xia, Junping Wang","doi":"10.1097/CAD.0000000000001701","DOIUrl":null,"url":null,"abstract":"<p><p>The combination of anlotinib with immune checkpoint inhibitors (ICIs) has become a common treatment modality in clinical practice. However, the optimal dose of anlotinib to use remains unclear. We collected patients with advanced non-small cell lung cancer (NSCLC) who received programmed cell death-1 blockade combined with different dose of anlotinib as second-line or later line therapy. Subsequently, the efficacy and safety of the combination therapy as well as subgroup analyses of different doses of anlotinib were analyzed. Cox regression was performed to analyze significant factors correlated with progression-free survival (PFS) and overall survival (OS). A total of 50 eligible patients with NSCLC who received anlotinib combined with ICIs therapy were included, of which 27 received low-dose anlotinib (8 mg), and 23 were administered high-dose anlotinib (12 mg). The median PFS (mPFS) and the median OS (mOS) for all patients were 8.3 months [95% confidence interval (CI): 6.3-10.3] and 17.6 months (95% CI: 16.5-18.7), respectively. Subgroup analyses showed that patients treated with 8 mg of anlotinib plus ICIs had significantly longer mPFS than those treated with 12 mg of anlotinib plus ICIs (8.7 vs 6.7 months, P = 0.016). The overall incidence of adverse events was 68.0%, and the most common adverse events of all grades were hypertension. Meanwhile, the incidence of adverse events was higher for 12 mg of anlotinib plus ICIs than that of 8 mg of anlotinib plus ICIs (82.6 vs 55.6%, P = 0.041). Low-dose anlotinib in combination with ICIs for advanced NSCLC may be an effective and well-tolerated option.</p>","PeriodicalId":7969,"journal":{"name":"Anti-Cancer Drugs","volume":" ","pages":"408-414"},"PeriodicalIF":2.2000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11969353/pdf/","citationCount":"0","resultStr":"{\"title\":\"Low-dose anlotinib plus immune checkpoint inhibitors offers better efficacy and safety in advanced non-small cell lung cancer treatment.\",\"authors\":\"Tingfei Tan, Siyu Yuan, Weiwei Chu, Jiemei Jiang, Meiling Chen, Quan Xia, Junping Wang\",\"doi\":\"10.1097/CAD.0000000000001701\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The combination of anlotinib with immune checkpoint inhibitors (ICIs) has become a common treatment modality in clinical practice. However, the optimal dose of anlotinib to use remains unclear. We collected patients with advanced non-small cell lung cancer (NSCLC) who received programmed cell death-1 blockade combined with different dose of anlotinib as second-line or later line therapy. Subsequently, the efficacy and safety of the combination therapy as well as subgroup analyses of different doses of anlotinib were analyzed. Cox regression was performed to analyze significant factors correlated with progression-free survival (PFS) and overall survival (OS). A total of 50 eligible patients with NSCLC who received anlotinib combined with ICIs therapy were included, of which 27 received low-dose anlotinib (8 mg), and 23 were administered high-dose anlotinib (12 mg). The median PFS (mPFS) and the median OS (mOS) for all patients were 8.3 months [95% confidence interval (CI): 6.3-10.3] and 17.6 months (95% CI: 16.5-18.7), respectively. Subgroup analyses showed that patients treated with 8 mg of anlotinib plus ICIs had significantly longer mPFS than those treated with 12 mg of anlotinib plus ICIs (8.7 vs 6.7 months, P = 0.016). The overall incidence of adverse events was 68.0%, and the most common adverse events of all grades were hypertension. Meanwhile, the incidence of adverse events was higher for 12 mg of anlotinib plus ICIs than that of 8 mg of anlotinib plus ICIs (82.6 vs 55.6%, P = 0.041). Low-dose anlotinib in combination with ICIs for advanced NSCLC may be an effective and well-tolerated option.</p>\",\"PeriodicalId\":7969,\"journal\":{\"name\":\"Anti-Cancer Drugs\",\"volume\":\" \",\"pages\":\"408-414\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11969353/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anti-Cancer Drugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/CAD.0000000000001701\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anti-Cancer Drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CAD.0000000000001701","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
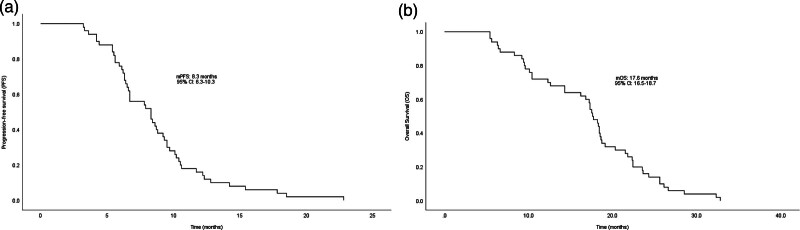
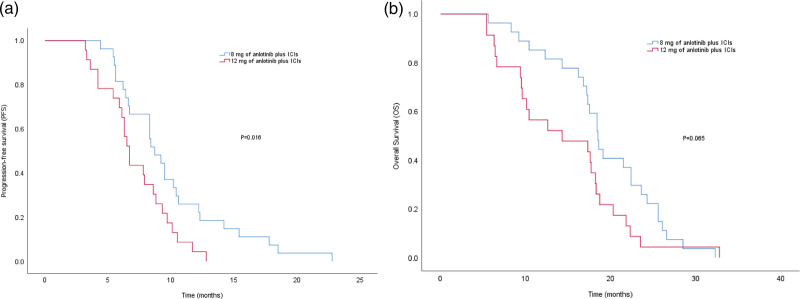
anlotinib联合免疫检查点抑制剂(ICIs)已成为临床常用的治疗方式。然而,使用安洛替尼的最佳剂量仍不清楚。我们收集了晚期非小细胞肺癌(NSCLC)患者,他们接受程序性细胞死亡-1阻断联合不同剂量的安洛替尼作为二线或后期治疗。随后,对联合治疗的疗效和安全性进行分析,并对不同剂量的安洛替尼进行亚组分析。采用Cox回归分析与无进展生存期(PFS)和总生存期(OS)相关的重要因素。共纳入50例接受安洛替尼联合ICIs治疗的符合条件的NSCLC患者,其中27例接受低剂量安洛替尼(8mg)治疗,23例接受高剂量安洛替尼(12mg)治疗。所有患者的中位PFS (mPFS)和中位OS (mOS)分别为8.3个月[95%可信区间(CI): 6.3-10.3]和17.6个月(95% CI: 16.5-18.7)。亚组分析显示,8 mg安洛替尼加ICIs治疗的患者mPFS明显长于12 mg安洛替尼加ICIs治疗的患者(8.7个月vs 6.7个月,P = 0.016)。总体不良事件发生率为68.0%,各级别最常见的不良事件为高血压。同时,12 mg安洛替尼加ICIs组不良事件发生率高于8 mg安洛替尼加ICIs组(82.6% vs 55.6%, P = 0.041)。低剂量anlotinib联合ICIs治疗晚期NSCLC可能是一种有效且耐受性良好的选择。
Low-dose anlotinib plus immune checkpoint inhibitors offers better efficacy and safety in advanced non-small cell lung cancer treatment.
The combination of anlotinib with immune checkpoint inhibitors (ICIs) has become a common treatment modality in clinical practice. However, the optimal dose of anlotinib to use remains unclear. We collected patients with advanced non-small cell lung cancer (NSCLC) who received programmed cell death-1 blockade combined with different dose of anlotinib as second-line or later line therapy. Subsequently, the efficacy and safety of the combination therapy as well as subgroup analyses of different doses of anlotinib were analyzed. Cox regression was performed to analyze significant factors correlated with progression-free survival (PFS) and overall survival (OS). A total of 50 eligible patients with NSCLC who received anlotinib combined with ICIs therapy were included, of which 27 received low-dose anlotinib (8 mg), and 23 were administered high-dose anlotinib (12 mg). The median PFS (mPFS) and the median OS (mOS) for all patients were 8.3 months [95% confidence interval (CI): 6.3-10.3] and 17.6 months (95% CI: 16.5-18.7), respectively. Subgroup analyses showed that patients treated with 8 mg of anlotinib plus ICIs had significantly longer mPFS than those treated with 12 mg of anlotinib plus ICIs (8.7 vs 6.7 months, P = 0.016). The overall incidence of adverse events was 68.0%, and the most common adverse events of all grades were hypertension. Meanwhile, the incidence of adverse events was higher for 12 mg of anlotinib plus ICIs than that of 8 mg of anlotinib plus ICIs (82.6 vs 55.6%, P = 0.041). Low-dose anlotinib in combination with ICIs for advanced NSCLC may be an effective and well-tolerated option.
期刊介绍:
Anti-Cancer Drugs reports both clinical and experimental results related to anti-cancer drugs, and welcomes contributions on anti-cancer drug design, drug delivery, pharmacology, hormonal and biological modalities and chemotherapy evaluation. An internationally refereed journal devoted to the fast publication of innovative investigations on therapeutic agents against cancer, Anti-Cancer Drugs aims to stimulate and report research on both toxic and non-toxic anti-cancer agents. Consequently, the scope on the journal will cover both conventional cytotoxic chemotherapy and hormonal or biological response modalities such as interleukins and immunotherapy. Submitted articles undergo a preliminary review by the editor. Some articles may be returned to authors without further consideration. Those being considered for publication will undergo further assessment and peer-review by the editors and those invited to do so from a reviewer pool.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


