Kjetil Fosse, Magnus Salomonsen, Sven Erik Gisvold, Bjørnar Gundersen, Trond Nordseth
{"title":"能插管,不能通气:一种处理插管后通气和氧合问题的算法。","authors":"Kjetil Fosse, Magnus Salomonsen, Sven Erik Gisvold, Bjørnar Gundersen, Trond Nordseth","doi":"10.1111/aas.70007","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and methods: </strong>Few guidelines address how to handle unanticipated ventilatory problems and hypoxemia in a successfully intubated patient. We will refer to this situation as \"can intubate-cannot ventilate.\" The situation may occur immediately after intubation or later during general anaesthesia. The aim of this paper is to describe an algorithm for handling this situation. In an intubated patient, the airway can be considered a continuum from the ventilator to the alveoli, and the problem is somewhere along this route: Ventilator → Hoses → Filter → Tracheal tube (TT) → Tracheae → Bronchi → Bronchioles → Alveoli. The proposed algorithm is based on clinical experience and has not been externally validated.</p><p><strong>Results: </strong>The first critical decision to be made is whether the TT has been placed correctly in the trachea or not. Positive wave-formed capnography is the primary marker for correct intubation. Video and/or direct laryngoscopy can be used for further verification. The patient should be disconnected from the ventilator and manually ventilated with bag-valve and 100% oxygen. An open tube should then be verified by applying a suction catheter through the tube. If these measures do not improve the situation, a fibreoptic scope should be inserted to further assess possible causes of difficult ventilation. If no obvious treatable cause is detected at this point, bronchospasm, anaphylaxis, or pneumothorax should be ruled out or treated. Further handling should focus on optimizing gas exchange in the lungs and considering more advanced treatment options to improve oxygenation and circulation.</p><p><strong>Conclusions: </strong>We have proposed an algorithm to handle unanticipated problems with ventilation and oxygenation in a patient who has been successfully intubated. Equipment failure and a blocked TT should be ruled out before diagnosing and treating medical or surgical causes of ventilatory problems.</p><p><strong>Editorial comment: </strong>This article presents a logical approach to the time-sensitive and critical situation where, for some reason, after intubation, ventilation of the lungs is not succeeding. The authors propose steps for a systematic approach, and recognition of different possible explanations for ventilation not working is informative.</p>","PeriodicalId":6909,"journal":{"name":"Acta Anaesthesiologica Scandinavica","volume":"69 3","pages":"e70007"},"PeriodicalIF":2.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11848235/pdf/","citationCount":"0","resultStr":"{\"title\":\"Can intubate, cannot ventilate: A proposed algorithm to handle problems with ventilation and oxygenation after intubation.\",\"authors\":\"Kjetil Fosse, Magnus Salomonsen, Sven Erik Gisvold, Bjørnar Gundersen, Trond Nordseth\",\"doi\":\"10.1111/aas.70007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and methods: </strong>Few guidelines address how to handle unanticipated ventilatory problems and hypoxemia in a successfully intubated patient. We will refer to this situation as \\\"can intubate-cannot ventilate.\\\" The situation may occur immediately after intubation or later during general anaesthesia. The aim of this paper is to describe an algorithm for handling this situation. In an intubated patient, the airway can be considered a continuum from the ventilator to the alveoli, and the problem is somewhere along this route: Ventilator → Hoses → Filter → Tracheal tube (TT) → Tracheae → Bronchi → Bronchioles → Alveoli. The proposed algorithm is based on clinical experience and has not been externally validated.</p><p><strong>Results: </strong>The first critical decision to be made is whether the TT has been placed correctly in the trachea or not. Positive wave-formed capnography is the primary marker for correct intubation. Video and/or direct laryngoscopy can be used for further verification. The patient should be disconnected from the ventilator and manually ventilated with bag-valve and 100% oxygen. An open tube should then be verified by applying a suction catheter through the tube. If these measures do not improve the situation, a fibreoptic scope should be inserted to further assess possible causes of difficult ventilation. If no obvious treatable cause is detected at this point, bronchospasm, anaphylaxis, or pneumothorax should be ruled out or treated. Further handling should focus on optimizing gas exchange in the lungs and considering more advanced treatment options to improve oxygenation and circulation.</p><p><strong>Conclusions: </strong>We have proposed an algorithm to handle unanticipated problems with ventilation and oxygenation in a patient who has been successfully intubated. Equipment failure and a blocked TT should be ruled out before diagnosing and treating medical or surgical causes of ventilatory problems.</p><p><strong>Editorial comment: </strong>This article presents a logical approach to the time-sensitive and critical situation where, for some reason, after intubation, ventilation of the lungs is not succeeding. The authors propose steps for a systematic approach, and recognition of different possible explanations for ventilation not working is informative.</p>\",\"PeriodicalId\":6909,\"journal\":{\"name\":\"Acta Anaesthesiologica Scandinavica\",\"volume\":\"69 3\",\"pages\":\"e70007\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11848235/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Anaesthesiologica Scandinavica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/aas.70007\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Anaesthesiologica Scandinavica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/aas.70007","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Can intubate, cannot ventilate: A proposed algorithm to handle problems with ventilation and oxygenation after intubation.
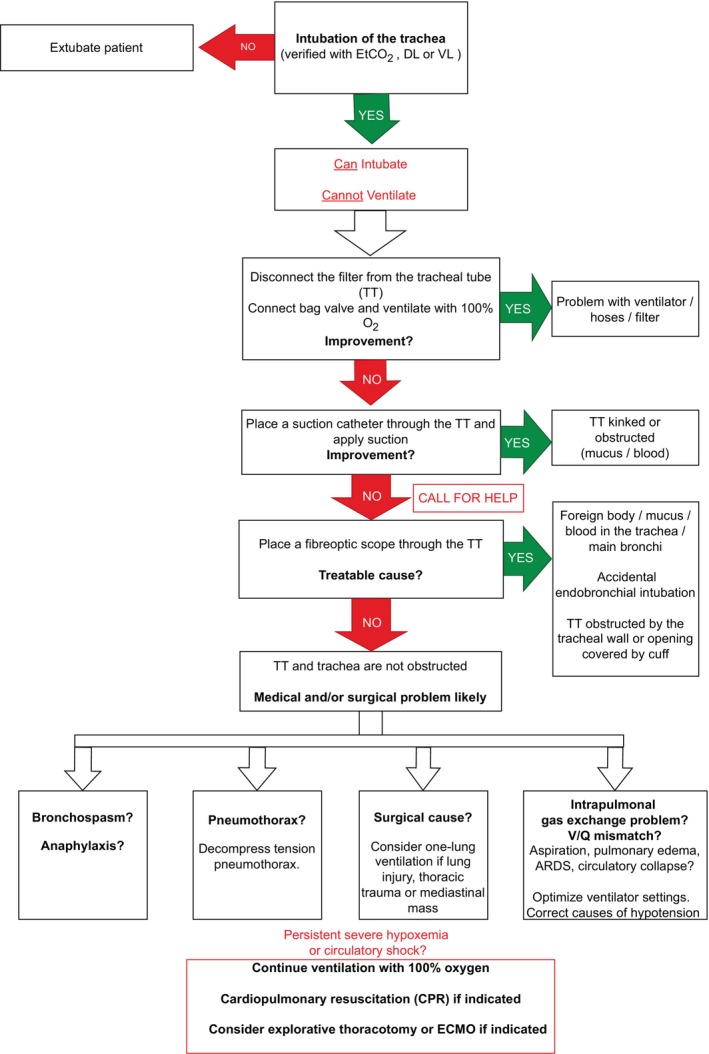
Background and methods: Few guidelines address how to handle unanticipated ventilatory problems and hypoxemia in a successfully intubated patient. We will refer to this situation as "can intubate-cannot ventilate." The situation may occur immediately after intubation or later during general anaesthesia. The aim of this paper is to describe an algorithm for handling this situation. In an intubated patient, the airway can be considered a continuum from the ventilator to the alveoli, and the problem is somewhere along this route: Ventilator → Hoses → Filter → Tracheal tube (TT) → Tracheae → Bronchi → Bronchioles → Alveoli. The proposed algorithm is based on clinical experience and has not been externally validated.
Results: The first critical decision to be made is whether the TT has been placed correctly in the trachea or not. Positive wave-formed capnography is the primary marker for correct intubation. Video and/or direct laryngoscopy can be used for further verification. The patient should be disconnected from the ventilator and manually ventilated with bag-valve and 100% oxygen. An open tube should then be verified by applying a suction catheter through the tube. If these measures do not improve the situation, a fibreoptic scope should be inserted to further assess possible causes of difficult ventilation. If no obvious treatable cause is detected at this point, bronchospasm, anaphylaxis, or pneumothorax should be ruled out or treated. Further handling should focus on optimizing gas exchange in the lungs and considering more advanced treatment options to improve oxygenation and circulation.
Conclusions: We have proposed an algorithm to handle unanticipated problems with ventilation and oxygenation in a patient who has been successfully intubated. Equipment failure and a blocked TT should be ruled out before diagnosing and treating medical or surgical causes of ventilatory problems.
Editorial comment: This article presents a logical approach to the time-sensitive and critical situation where, for some reason, after intubation, ventilation of the lungs is not succeeding. The authors propose steps for a systematic approach, and recognition of different possible explanations for ventilation not working is informative.
期刊介绍:
Acta Anaesthesiologica Scandinavica publishes papers on original work in the fields of anaesthesiology, intensive care, pain, emergency medicine, and subjects related to their basic sciences, on condition that they are contributed exclusively to this Journal. Case reports and short communications may be considered for publication if of particular interest; also letters to the Editor, especially if related to already published material. The editorial board is free to discuss the publication of reviews on current topics, the choice of which, however, is the prerogative of the board. Every effort will be made by the Editors and selected experts to expedite a critical review of manuscripts in order to ensure rapid publication of papers of a high scientific standard.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


