Yosef Ellenbogen, Shervin Taslimi, Jonas Shellenberger, Susan B Brogly, Gelareh Zadeh, Ryan Alkins
{"title":"胶质母细胞瘤的临终关怀:一项基于人群的研究。","authors":"Yosef Ellenbogen, Shervin Taslimi, Jonas Shellenberger, Susan B Brogly, Gelareh Zadeh, Ryan Alkins","doi":"10.1093/neuonc/noaf043","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The end-of-life (EoL) phase of care is inevitable for glioblastoma (GBM) patients; however, it lacks standardization. This study aimed to characterize the utilization of care at EoL in GBM patients, focusing on trends over time, regional variability, and the influence of socioeconomic factors.</p><p><strong>Methods: </strong>This was a retrospective population-based cohort study of all patients with GBM treated in Ontario between 1994 and 2018 using administrative health data and registries available at ICES (formerly the Institute for Clinical Evaluative Sciences). The proportion of patients with palliative care, supportive care, and in-hospital deaths by year of diagnosis was estimated, and trends were assessed with the Cochrane-Armitage trend test.</p><p><strong>Results: </strong>The cohort included 9013 GBM patients. There was an increase in supportive care components over the study time period (29.6% in 1994-1998 to 60.2% in 2014-2018; P < .0001). There was a simultaneous decrease in in-hospital deaths (50.5% in 1994-1998 to 21.4% in 2014-2018; P < .001) and hospitalizations within 30 days before death (65.5% in 1994-1998 to 51.7% in 2014-2018, P < .001). This coincided with an increase in chemotherapy administration within 14 days of death and intensive care unit admissions within 30 days of death over the studied period of time. Patient neighborhood income level and geographic location influenced EoL care patterns with regard to both supportive and aggressive components.</p><p><strong>Conclusions: </strong>Over time there was an expansion of both inpatient and outpatient palliative care use at EoL. Rurality and neighborhood income quintile significantly influenced the utilization of these resources, underscoring the need for standardized EoL care practices.</p>","PeriodicalId":19377,"journal":{"name":"Neuro-oncology","volume":" ","pages":"1640-1653"},"PeriodicalIF":13.4000,"publicationDate":"2025-07-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12309700/pdf/","citationCount":"0","resultStr":"{\"title\":\"End-of-life care in glioblastoma: A population-based study.\",\"authors\":\"Yosef Ellenbogen, Shervin Taslimi, Jonas Shellenberger, Susan B Brogly, Gelareh Zadeh, Ryan Alkins\",\"doi\":\"10.1093/neuonc/noaf043\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The end-of-life (EoL) phase of care is inevitable for glioblastoma (GBM) patients; however, it lacks standardization. This study aimed to characterize the utilization of care at EoL in GBM patients, focusing on trends over time, regional variability, and the influence of socioeconomic factors.</p><p><strong>Methods: </strong>This was a retrospective population-based cohort study of all patients with GBM treated in Ontario between 1994 and 2018 using administrative health data and registries available at ICES (formerly the Institute for Clinical Evaluative Sciences). The proportion of patients with palliative care, supportive care, and in-hospital deaths by year of diagnosis was estimated, and trends were assessed with the Cochrane-Armitage trend test.</p><p><strong>Results: </strong>The cohort included 9013 GBM patients. There was an increase in supportive care components over the study time period (29.6% in 1994-1998 to 60.2% in 2014-2018; P < .0001). There was a simultaneous decrease in in-hospital deaths (50.5% in 1994-1998 to 21.4% in 2014-2018; P < .001) and hospitalizations within 30 days before death (65.5% in 1994-1998 to 51.7% in 2014-2018, P < .001). This coincided with an increase in chemotherapy administration within 14 days of death and intensive care unit admissions within 30 days of death over the studied period of time. Patient neighborhood income level and geographic location influenced EoL care patterns with regard to both supportive and aggressive components.</p><p><strong>Conclusions: </strong>Over time there was an expansion of both inpatient and outpatient palliative care use at EoL. Rurality and neighborhood income quintile significantly influenced the utilization of these resources, underscoring the need for standardized EoL care practices.</p>\",\"PeriodicalId\":19377,\"journal\":{\"name\":\"Neuro-oncology\",\"volume\":\" \",\"pages\":\"1640-1653\"},\"PeriodicalIF\":13.4000,\"publicationDate\":\"2025-07-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12309700/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neuro-oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/neuonc/noaf043\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuro-oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/neuonc/noaf043","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
End-of-life care in glioblastoma: A population-based study.
Background: The end-of-life (EoL) phase of care is inevitable for glioblastoma (GBM) patients; however, it lacks standardization. This study aimed to characterize the utilization of care at EoL in GBM patients, focusing on trends over time, regional variability, and the influence of socioeconomic factors.
Methods: This was a retrospective population-based cohort study of all patients with GBM treated in Ontario between 1994 and 2018 using administrative health data and registries available at ICES (formerly the Institute for Clinical Evaluative Sciences). The proportion of patients with palliative care, supportive care, and in-hospital deaths by year of diagnosis was estimated, and trends were assessed with the Cochrane-Armitage trend test.
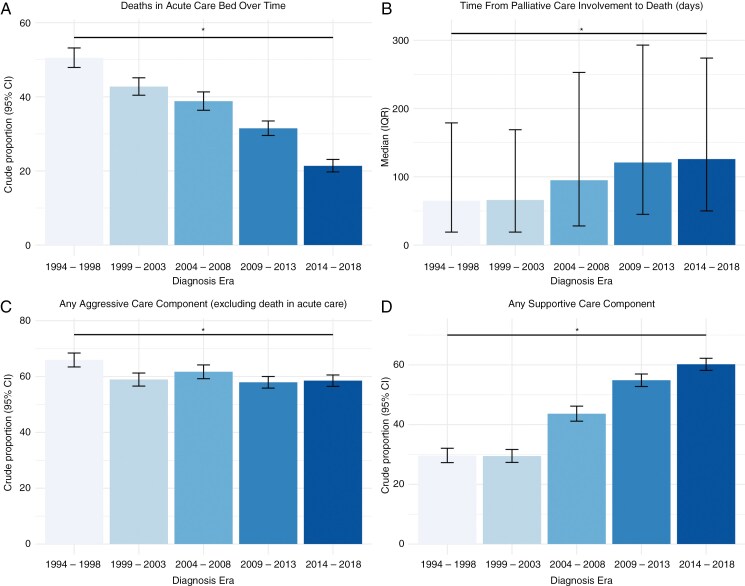
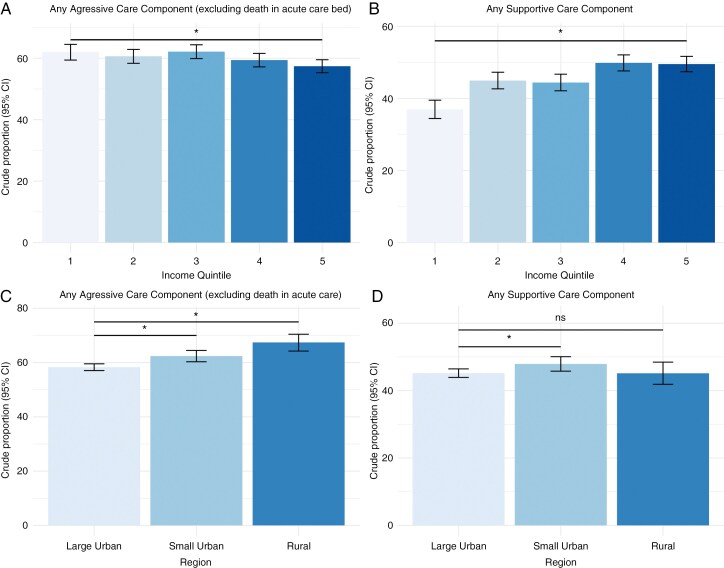
Results: The cohort included 9013 GBM patients. There was an increase in supportive care components over the study time period (29.6% in 1994-1998 to 60.2% in 2014-2018; P < .0001). There was a simultaneous decrease in in-hospital deaths (50.5% in 1994-1998 to 21.4% in 2014-2018; P < .001) and hospitalizations within 30 days before death (65.5% in 1994-1998 to 51.7% in 2014-2018, P < .001). This coincided with an increase in chemotherapy administration within 14 days of death and intensive care unit admissions within 30 days of death over the studied period of time. Patient neighborhood income level and geographic location influenced EoL care patterns with regard to both supportive and aggressive components.
Conclusions: Over time there was an expansion of both inpatient and outpatient palliative care use at EoL. Rurality and neighborhood income quintile significantly influenced the utilization of these resources, underscoring the need for standardized EoL care practices.
期刊介绍:
Neuro-Oncology, the official journal of the Society for Neuro-Oncology, has been published monthly since January 2010. Affiliated with the Japan Society for Neuro-Oncology and the European Association of Neuro-Oncology, it is a global leader in the field.
The journal is committed to swiftly disseminating high-quality information across all areas of neuro-oncology. It features peer-reviewed articles, reviews, symposia on various topics, abstracts from annual meetings, and updates from neuro-oncology societies worldwide.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


