{"title":"双侧腰椎显微减压后腰椎滑脱和脊柱侧凸进展及相关翻修率。","authors":"Walter-Soon-Yaw Wong, Ashton Kai Shun Tan, Kenneth Zhi Kuan Loi, Dhivakaran Gengatharan, Craigven Hao Sheng Sim, Hao Bin Chen, Yilun Huang","doi":"10.22603/ssrr.2024-0137","DOIUrl":null,"url":null,"abstract":"<p><p>Lumbar spine microscopic decompression (LSMD) is a common surgical procedure for decompressing neural elements. Although the optimal extent of decompression remains a critical consideration, limited evidence-based guidelines define the threshold for instrumented fusion to maintain biomechanical stability. Existing studies suggest that unilateral LSMD generally does not result in iatrogenic instability. However, the potential instability associated with bilateral segmental decompression (BLSMD) is less well-defined, particularly in patients with pre-existing degenerative lumbar scoliosis (SC) or spondylolisthesis (SL). This retrospective study included patients undergoing BLSMD without instrumented fusion. Pre-existing SC was defined as Cobb's angle ≥10° and SL as any anterior-posterior slip of operated level adjacent vertebral bodies. The primary outcome was new or progressive SC/SL measured on pre and postoperative radiographs. Secondary outcomes were revision rates, changes in Visual Analog Scores (bVAS/lVAS), and Oswestry Disability Index (ODI) scores, collected preoperatively and 1-2 years postoperatively. Baseline characteristics such as age, BMI, sex, and number of levels operated were also collected. A total of 31 patients were reviewed comprising 15 female and 16 male patients with a mean age of 61.4 years (21-78) and BMI of 26.5 (18-41). There were 14 one-level, 12 two-level, and 4 three-level BLSMD performed. Patients with pre-existing SC and SL had a 66% and 23% incidence of radiological progression, respectively, compared to 0% in patients without pre-existing deformity. Progression cases were associated with high reoperation rates (up to 75%) and seemed to have inferior clinical outcomes than those without progression. In patients undergoing BLSMD, pre-existing SC/SL is linked to a higher incidence of radiological progression and higher reoperation rates. For patients with SC/SL, careful consideration should be given to limiting decompression, potentially exploring fusion options, and implementing close postoperative radiographic monitoring.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"9 1","pages":"30-35"},"PeriodicalIF":1.2000,"publicationDate":"2024-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11808231/pdf/","citationCount":"0","resultStr":"{\"title\":\"Spondylolisthesis and Scoliosis Progression and Associated Revision Rates Following Bilateral Lumbar Spine Microscopic Decompression.\",\"authors\":\"Walter-Soon-Yaw Wong, Ashton Kai Shun Tan, Kenneth Zhi Kuan Loi, Dhivakaran Gengatharan, Craigven Hao Sheng Sim, Hao Bin Chen, Yilun Huang\",\"doi\":\"10.22603/ssrr.2024-0137\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Lumbar spine microscopic decompression (LSMD) is a common surgical procedure for decompressing neural elements. Although the optimal extent of decompression remains a critical consideration, limited evidence-based guidelines define the threshold for instrumented fusion to maintain biomechanical stability. Existing studies suggest that unilateral LSMD generally does not result in iatrogenic instability. However, the potential instability associated with bilateral segmental decompression (BLSMD) is less well-defined, particularly in patients with pre-existing degenerative lumbar scoliosis (SC) or spondylolisthesis (SL). This retrospective study included patients undergoing BLSMD without instrumented fusion. Pre-existing SC was defined as Cobb's angle ≥10° and SL as any anterior-posterior slip of operated level adjacent vertebral bodies. The primary outcome was new or progressive SC/SL measured on pre and postoperative radiographs. Secondary outcomes were revision rates, changes in Visual Analog Scores (bVAS/lVAS), and Oswestry Disability Index (ODI) scores, collected preoperatively and 1-2 years postoperatively. Baseline characteristics such as age, BMI, sex, and number of levels operated were also collected. A total of 31 patients were reviewed comprising 15 female and 16 male patients with a mean age of 61.4 years (21-78) and BMI of 26.5 (18-41). There were 14 one-level, 12 two-level, and 4 three-level BLSMD performed. Patients with pre-existing SC and SL had a 66% and 23% incidence of radiological progression, respectively, compared to 0% in patients without pre-existing deformity. Progression cases were associated with high reoperation rates (up to 75%) and seemed to have inferior clinical outcomes than those without progression. In patients undergoing BLSMD, pre-existing SC/SL is linked to a higher incidence of radiological progression and higher reoperation rates. For patients with SC/SL, careful consideration should be given to limiting decompression, potentially exploring fusion options, and implementing close postoperative radiographic monitoring.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"9 1\",\"pages\":\"30-35\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2024-08-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11808231/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2024-0137\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/27 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0137","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Spondylolisthesis and Scoliosis Progression and Associated Revision Rates Following Bilateral Lumbar Spine Microscopic Decompression.
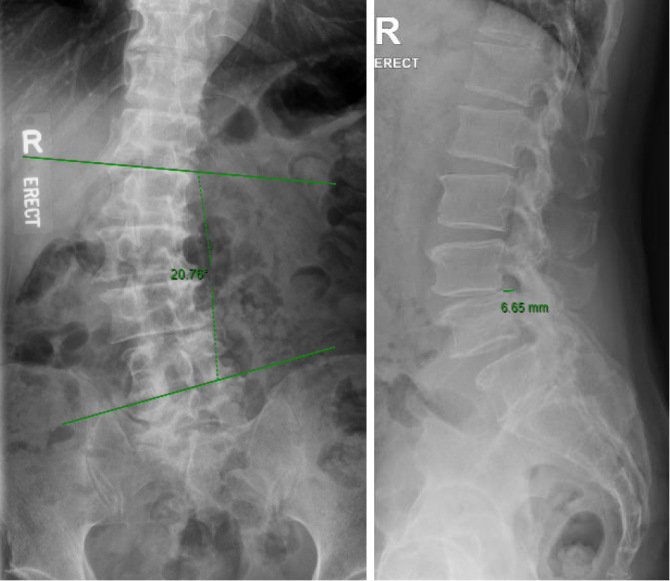
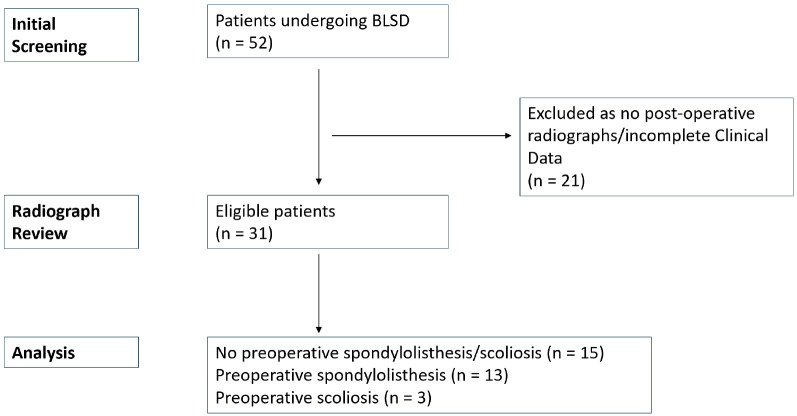
Lumbar spine microscopic decompression (LSMD) is a common surgical procedure for decompressing neural elements. Although the optimal extent of decompression remains a critical consideration, limited evidence-based guidelines define the threshold for instrumented fusion to maintain biomechanical stability. Existing studies suggest that unilateral LSMD generally does not result in iatrogenic instability. However, the potential instability associated with bilateral segmental decompression (BLSMD) is less well-defined, particularly in patients with pre-existing degenerative lumbar scoliosis (SC) or spondylolisthesis (SL). This retrospective study included patients undergoing BLSMD without instrumented fusion. Pre-existing SC was defined as Cobb's angle ≥10° and SL as any anterior-posterior slip of operated level adjacent vertebral bodies. The primary outcome was new or progressive SC/SL measured on pre and postoperative radiographs. Secondary outcomes were revision rates, changes in Visual Analog Scores (bVAS/lVAS), and Oswestry Disability Index (ODI) scores, collected preoperatively and 1-2 years postoperatively. Baseline characteristics such as age, BMI, sex, and number of levels operated were also collected. A total of 31 patients were reviewed comprising 15 female and 16 male patients with a mean age of 61.4 years (21-78) and BMI of 26.5 (18-41). There were 14 one-level, 12 two-level, and 4 three-level BLSMD performed. Patients with pre-existing SC and SL had a 66% and 23% incidence of radiological progression, respectively, compared to 0% in patients without pre-existing deformity. Progression cases were associated with high reoperation rates (up to 75%) and seemed to have inferior clinical outcomes than those without progression. In patients undergoing BLSMD, pre-existing SC/SL is linked to a higher incidence of radiological progression and higher reoperation rates. For patients with SC/SL, careful consideration should be given to limiting decompression, potentially exploring fusion options, and implementing close postoperative radiographic monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


