Erin Sullivan BS, Rebecca Schulte MPH, Michael B. Rothberg MD, MPH
{"title":"非感染住院患者使用皮质类固醇后白细胞计数升高","authors":"Erin Sullivan BS, Rebecca Schulte MPH, Michael B. Rothberg MD, MPH","doi":"10.1002/jhm.70008","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>It is widely accepted that corticosteroids cause leukocytosis. Clinicians must decide whether a rise in white blood cell (WBC) count is due to steroids versus other processes like developing infection.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>The objective of this study is to measure the increase in white blood cell count after corticosteroid administration in hospitalized patients without malignancy, infection, or immune dysfunction.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This is a retrospective cohort study from 2017 to 2018 in a single large healthcare system. We analyzed the trajectory of WBC count stratified by steroid dose. The study included nonsurgical patients admitted with at least two complete blood count measurements. Patients were excluded if they had immunosuppression, infection, malignancy, or steroid use within 2 weeks before admission. The main outcome was mean WBC count by day following corticosteroid administration.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Our sample included 28,425 patients with at least two WBC measurements, 1608 (5.7%) of which received steroids. WBC response peaked at 48 h after steroid administration with a mean increase of 2.4 × 10<sup>9</sup>/L WBCs. In all patients on steroids, across doses, the mean increase was 0.3 × 10<sup>9</sup>/L WBCs, 1.7 × 10<sup>9</sup>/L WBCs, and 4.84 × 10<sup>9</sup>/L WBCs in low, medium, and high dose groups, respectively. For patients not on steroids, the mean WBC count decreased during hospitalization.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>When interpreting WBC counts after initiating steroids, increases of up to 4.84 × 10<sup>9</sup>/L cells may be seen within 48 h after high-dose steroids. Larger increases, and any increase after low-dose steroids, suggest other causes of leukocytosis.</p>\n </section>\n </div>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"20 8","pages":"824-828"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.70008","citationCount":"0","resultStr":"{\"title\":\"Elevation in white blood cell count after corticosteroid use in noninfected hospitalized patients\",\"authors\":\"Erin Sullivan BS, Rebecca Schulte MPH, Michael B. Rothberg MD, MPH\",\"doi\":\"10.1002/jhm.70008\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>It is widely accepted that corticosteroids cause leukocytosis. Clinicians must decide whether a rise in white blood cell (WBC) count is due to steroids versus other processes like developing infection.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>The objective of this study is to measure the increase in white blood cell count after corticosteroid administration in hospitalized patients without malignancy, infection, or immune dysfunction.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This is a retrospective cohort study from 2017 to 2018 in a single large healthcare system. We analyzed the trajectory of WBC count stratified by steroid dose. The study included nonsurgical patients admitted with at least two complete blood count measurements. Patients were excluded if they had immunosuppression, infection, malignancy, or steroid use within 2 weeks before admission. The main outcome was mean WBC count by day following corticosteroid administration.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Our sample included 28,425 patients with at least two WBC measurements, 1608 (5.7%) of which received steroids. WBC response peaked at 48 h after steroid administration with a mean increase of 2.4 × 10<sup>9</sup>/L WBCs. In all patients on steroids, across doses, the mean increase was 0.3 × 10<sup>9</sup>/L WBCs, 1.7 × 10<sup>9</sup>/L WBCs, and 4.84 × 10<sup>9</sup>/L WBCs in low, medium, and high dose groups, respectively. For patients not on steroids, the mean WBC count decreased during hospitalization.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>When interpreting WBC counts after initiating steroids, increases of up to 4.84 × 10<sup>9</sup>/L cells may be seen within 48 h after high-dose steroids. Larger increases, and any increase after low-dose steroids, suggest other causes of leukocytosis.</p>\\n </section>\\n </div>\",\"PeriodicalId\":15883,\"journal\":{\"name\":\"Journal of hospital medicine\",\"volume\":\"20 8\",\"pages\":\"824-828\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-02-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.70008\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of hospital medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.70008\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.70008","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Elevation in white blood cell count after corticosteroid use in noninfected hospitalized patients
Background
It is widely accepted that corticosteroids cause leukocytosis. Clinicians must decide whether a rise in white blood cell (WBC) count is due to steroids versus other processes like developing infection.
Objective
The objective of this study is to measure the increase in white blood cell count after corticosteroid administration in hospitalized patients without malignancy, infection, or immune dysfunction.
Methods
This is a retrospective cohort study from 2017 to 2018 in a single large healthcare system. We analyzed the trajectory of WBC count stratified by steroid dose. The study included nonsurgical patients admitted with at least two complete blood count measurements. Patients were excluded if they had immunosuppression, infection, malignancy, or steroid use within 2 weeks before admission. The main outcome was mean WBC count by day following corticosteroid administration.
Results
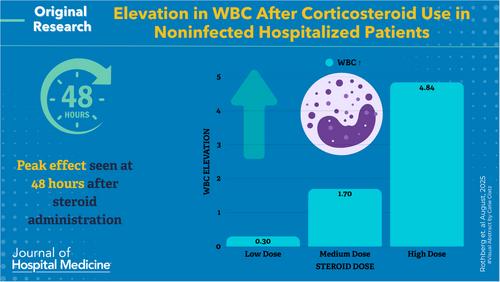
Our sample included 28,425 patients with at least two WBC measurements, 1608 (5.7%) of which received steroids. WBC response peaked at 48 h after steroid administration with a mean increase of 2.4 × 109/L WBCs. In all patients on steroids, across doses, the mean increase was 0.3 × 109/L WBCs, 1.7 × 109/L WBCs, and 4.84 × 109/L WBCs in low, medium, and high dose groups, respectively. For patients not on steroids, the mean WBC count decreased during hospitalization.
Conclusions
When interpreting WBC counts after initiating steroids, increases of up to 4.84 × 109/L cells may be seen within 48 h after high-dose steroids. Larger increases, and any increase after low-dose steroids, suggest other causes of leukocytosis.
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


