Carrie R. Howell PhD, Shiori Tanaka PhD, Li Zhang MS, April P. Carson PhD, Nengjun Yi PhD, James M. Shikany DrPH, W. Timothy Garvey MD, Andrea L. Cherrington MD
{"title":"在等式中加入健康的社会决定因素:利用临床和健康的社会决定因素来预测2型糖尿病的心脏代谢疾病分期模型的发展。","authors":"Carrie R. Howell PhD, Shiori Tanaka PhD, Li Zhang MS, April P. Carson PhD, Nengjun Yi PhD, James M. Shikany DrPH, W. Timothy Garvey MD, Andrea L. Cherrington MD","doi":"10.1111/dom.16241","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>Identifying individuals at the highest risk of progression to type 2 diabetes (T2D) using clinical and social determinants of health (SDoH) measures will help prioritize prevention efforts. We aimed to investigate model performance after adding SDoH to a previously validated cardiometabolic disease staging diabetes risk prediction model.</p>\n </section>\n \n <section>\n \n <h3> Materials and Methods</h3>\n \n <p>We developed a Bayesian predictive model using data [clinical factors: fasting glucose, blood pressure, body mass index, high-density lipoprotein cholesterol, triglycerides; individual SDoH: income, education, health insurance status, relationship status, self-reported stress and neighbourhood SDoH: census-tract level social vulnerability index] from the REasons for Geographic And Racial Differences in Stroke (REGARDS) study to predict T2D with external validation using the Coronary Artery Risk Development in Young Adults (CARDIA) study.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The analysis included 9907 REGARDS participants without T2D at baseline [mean age 63 years (SD 8.5), 54% female, 33% non-Hispanic Black] who completed a follow-up visit 10 years later. <i>N</i> = 1268 (12.8%) developed T2D. Adding SDoH to the clinical model modestly improved performance [Area Under the Curve: 0.802 vs. 0.804, <i>p</i> = 0.01]. Calibration plots indicated that the clinical model underpredicted risk in disadvantaged SDoH subgroups, whereas the clinical plus SDoH model improved prediction accuracy in subgroups. Classification tables revealed that the clinical plus SDoH model accurately reclassified individuals categorized as borderline risk in a clinical-only model.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Including SDoH in T2D risk prediction and stratification at the population level may aid in better classifying T2D risk among vulnerable populations, which has important implications for screening strategies.</p>\n </section>\n </div>","PeriodicalId":158,"journal":{"name":"Diabetes, Obesity & Metabolism","volume":"27 5","pages":"2454-2462"},"PeriodicalIF":5.7000,"publicationDate":"2025-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dom.16241","citationCount":"0","resultStr":"{\"title\":\"Adding social determinants of health to the equation: Development of a cardiometabolic disease staging model using clinical and social determinants of health to predict type 2 diabetes\",\"authors\":\"Carrie R. Howell PhD, Shiori Tanaka PhD, Li Zhang MS, April P. Carson PhD, Nengjun Yi PhD, James M. Shikany DrPH, W. Timothy Garvey MD, Andrea L. Cherrington MD\",\"doi\":\"10.1111/dom.16241\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Identifying individuals at the highest risk of progression to type 2 diabetes (T2D) using clinical and social determinants of health (SDoH) measures will help prioritize prevention efforts. We aimed to investigate model performance after adding SDoH to a previously validated cardiometabolic disease staging diabetes risk prediction model.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Materials and Methods</h3>\\n \\n <p>We developed a Bayesian predictive model using data [clinical factors: fasting glucose, blood pressure, body mass index, high-density lipoprotein cholesterol, triglycerides; individual SDoH: income, education, health insurance status, relationship status, self-reported stress and neighbourhood SDoH: census-tract level social vulnerability index] from the REasons for Geographic And Racial Differences in Stroke (REGARDS) study to predict T2D with external validation using the Coronary Artery Risk Development in Young Adults (CARDIA) study.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The analysis included 9907 REGARDS participants without T2D at baseline [mean age 63 years (SD 8.5), 54% female, 33% non-Hispanic Black] who completed a follow-up visit 10 years later. <i>N</i> = 1268 (12.8%) developed T2D. Adding SDoH to the clinical model modestly improved performance [Area Under the Curve: 0.802 vs. 0.804, <i>p</i> = 0.01]. Calibration plots indicated that the clinical model underpredicted risk in disadvantaged SDoH subgroups, whereas the clinical plus SDoH model improved prediction accuracy in subgroups. Classification tables revealed that the clinical plus SDoH model accurately reclassified individuals categorized as borderline risk in a clinical-only model.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Including SDoH in T2D risk prediction and stratification at the population level may aid in better classifying T2D risk among vulnerable populations, which has important implications for screening strategies.</p>\\n </section>\\n </div>\",\"PeriodicalId\":158,\"journal\":{\"name\":\"Diabetes, Obesity & Metabolism\",\"volume\":\"27 5\",\"pages\":\"2454-2462\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2025-02-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dom.16241\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes, Obesity & Metabolism\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/dom.16241\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes, Obesity & Metabolism","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/dom.16241","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
目的:使用临床和社会健康决定因素(SDoH)措施确定进展为2型糖尿病(T2D)风险最高的个体将有助于优先考虑预防工作。我们的目的是在先前验证的心脏代谢疾病分期糖尿病风险预测模型中加入SDoH后研究模型的性能。材料与方法:利用临床因素:空腹血糖、血压、体重指数、高密度脂蛋白胆固醇、甘油三酯等数据建立贝叶斯预测模型;个人SDoH:收入、教育、健康保险状况、关系状况、自我报告的压力和社区SDoH:人口普查水平的社会脆弱性指数],来自中风地理和种族差异的原因(REGARDS)研究,通过外部验证预测年轻人冠状动脉风险发展(CARDIA)研究的T2D。结果:分析包括9907名基线时无T2D的REGARDS参与者[平均年龄63岁(SD 8.5), 54%为女性,33%为非西班牙裔黑人],他们在10年后完成了随访。1268例(12.8%)发生T2D。在临床模型中加入SDoH可适度改善性能[曲线下面积:0.802 vs. 0.804, p = 0.01]。校正图显示,临床模型低估了弱势SDoH亚组的风险,而临床加SDoH模型提高了亚组的预测准确性。分类表显示,临床加SDoH模型准确地重新分类了在仅临床模型中被归类为边缘风险的个体。结论:将SDoH纳入T2D风险预测和人群分层中,有助于更好地对弱势人群进行T2D风险分类,对筛查策略具有重要意义。
Adding social determinants of health to the equation: Development of a cardiometabolic disease staging model using clinical and social determinants of health to predict type 2 diabetes
Aims
Identifying individuals at the highest risk of progression to type 2 diabetes (T2D) using clinical and social determinants of health (SDoH) measures will help prioritize prevention efforts. We aimed to investigate model performance after adding SDoH to a previously validated cardiometabolic disease staging diabetes risk prediction model.
Materials and Methods
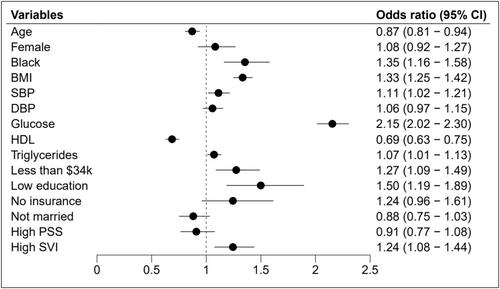
We developed a Bayesian predictive model using data [clinical factors: fasting glucose, blood pressure, body mass index, high-density lipoprotein cholesterol, triglycerides; individual SDoH: income, education, health insurance status, relationship status, self-reported stress and neighbourhood SDoH: census-tract level social vulnerability index] from the REasons for Geographic And Racial Differences in Stroke (REGARDS) study to predict T2D with external validation using the Coronary Artery Risk Development in Young Adults (CARDIA) study.
Results
The analysis included 9907 REGARDS participants without T2D at baseline [mean age 63 years (SD 8.5), 54% female, 33% non-Hispanic Black] who completed a follow-up visit 10 years later. N = 1268 (12.8%) developed T2D. Adding SDoH to the clinical model modestly improved performance [Area Under the Curve: 0.802 vs. 0.804, p = 0.01]. Calibration plots indicated that the clinical model underpredicted risk in disadvantaged SDoH subgroups, whereas the clinical plus SDoH model improved prediction accuracy in subgroups. Classification tables revealed that the clinical plus SDoH model accurately reclassified individuals categorized as borderline risk in a clinical-only model.
Conclusion
Including SDoH in T2D risk prediction and stratification at the population level may aid in better classifying T2D risk among vulnerable populations, which has important implications for screening strategies.
期刊介绍:
Diabetes, Obesity and Metabolism is primarily a journal of clinical and experimental pharmacology and therapeutics covering the interrelated areas of diabetes, obesity and metabolism. The journal prioritises high-quality original research that reports on the effects of new or existing therapies, including dietary, exercise and lifestyle (non-pharmacological) interventions, in any aspect of metabolic and endocrine disease, either in humans or animal and cellular systems. ‘Metabolism’ may relate to lipids, bone and drug metabolism, or broader aspects of endocrine dysfunction. Preclinical pharmacology, pharmacokinetic studies, meta-analyses and those addressing drug safety and tolerability are also highly suitable for publication in this journal. Original research may be published as a main paper or as a research letter.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


