{"title":"在南非约翰内斯堡克里斯·哈尼·巴拉格瓦纳特学术医院重症监护室使用静脉注射免疫球蛋白治疗重症COVID-19。","authors":"G Mensky, A van Blydenstein, J Damelin, S Omar","doi":"10.7196/SAJCC.2024.v40i3.1897","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>COVID-19 infection has a variable clinical presentation, with a small subgroup of patients developing severe disease, requiring intensive care with mechanical ventilation, with an increased mortality rate. South Africa (SA) has experienced multiple waves of this pandemic, spanning the pre-vaccine and vaccine periods. The method and initiation of treatment is a debated topic, changing according to evolving research and the literature. The present study investigated the use of high-dose intravenous immunoglobulin (IVIg) as a salvage therapy after initial medical treatment failure.</p><p><strong>Objectives: </strong>To compare disease progression among critically ill COVID-19 pneumonia patients receiving IVIg therapy with that in patients receiving standard of care (SoC), in respect of inflammation, organ dysfunction and oxygenation.</p><p><strong>Methods: </strong>This was a single-centre, retrospective study of patients admitted to the intensive care unit (ICU) at Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, during the pre-vaccine COVID-19 pandemic. Demographics, inflammatory markers (C-reactive protein (CRP)), organ function (Sequential Organ Failure Assessment (SOFA) score), oxygenation (ratio of partial pressure of oxygen in arterial blood to fraction of inspiratory oxygen (P/F ratio)), overall mortality and complications (nosocomial infections and thromboembolism) were recorded and compared.</p><p><strong>Results: </strong>We included 113 eligible patients in the study. The IVIg cohort had a significantly lower initial P/F ratio than the SoC cohort (p=0.01), but the change in P/F ratio was similar (p=0.54). Initial CRP and changes in CRP were similar in the two groups (p=0.38 and p=0.75, respectively), as were initial SOFA score and changes in SOFA score (p=0.18 and p=0.08, respectively) and vasopressor dose on day 0 and day 5 (p=0.97 and p=0.93, respectively). Duration of mechanical ventilation did not differ significantly between the IVIg group and the SoC group (p=0.13). There were no significant differences in measured complications between the two groups. On univariate analysis, the relative risk of death was 1.6 times higher (95% confidence interval (CI) 1.1 - 2.3) in the IVIg group; however, a logistical regression model demonstrated that only a higher P/F ratio (odds ratio (OR) 0.991; 95% CI 0.983 - 0.997) and higher mean airway pressure (OR 1.283; 95% CI 1.026 - 1.604) were significantly associated with ICU mortality.</p><p><strong>Conclusion: </strong>Use of IVIg in our study was directed at an older population, with significantly worse oxygenation. We found no evidence of adverse effects of immunoglobulin therapy; however, we found no benefit either. Only the P/F ratio and mean airway pressure independently predicted ICU mortality.</p><p><strong>Contribution of the study: </strong>During the COVID-19 pandemic, treatment protocols changed in response to the evolving literature. Hospitals were faced with choosing a treatment modality that they believed at the time had benefit. Chris Hani Baragwanath Hospital in Johannesburg, South Africa (SA), incorporated IVIg into its treatment protocols for patients with severe COVID pneumonia requiring ICU admission. This study retrospectively analysed the use of IVIg therapy in the hope of creating a more robust understanding of its safety and efficacy as a treatment option for SA patients in the future.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"40 3","pages":"e1897"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11792588/pdf/","citationCount":"0","resultStr":"{\"title\":\"Use of intravenous immunoglobulin for the treatment of severe COVID-19 in the Chris Hani Baragwanath Academic Hospital intensive care unit, Johannesburg, South Africa.\",\"authors\":\"G Mensky, A van Blydenstein, J Damelin, S Omar\",\"doi\":\"10.7196/SAJCC.2024.v40i3.1897\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>COVID-19 infection has a variable clinical presentation, with a small subgroup of patients developing severe disease, requiring intensive care with mechanical ventilation, with an increased mortality rate. South Africa (SA) has experienced multiple waves of this pandemic, spanning the pre-vaccine and vaccine periods. The method and initiation of treatment is a debated topic, changing according to evolving research and the literature. The present study investigated the use of high-dose intravenous immunoglobulin (IVIg) as a salvage therapy after initial medical treatment failure.</p><p><strong>Objectives: </strong>To compare disease progression among critically ill COVID-19 pneumonia patients receiving IVIg therapy with that in patients receiving standard of care (SoC), in respect of inflammation, organ dysfunction and oxygenation.</p><p><strong>Methods: </strong>This was a single-centre, retrospective study of patients admitted to the intensive care unit (ICU) at Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, during the pre-vaccine COVID-19 pandemic. Demographics, inflammatory markers (C-reactive protein (CRP)), organ function (Sequential Organ Failure Assessment (SOFA) score), oxygenation (ratio of partial pressure of oxygen in arterial blood to fraction of inspiratory oxygen (P/F ratio)), overall mortality and complications (nosocomial infections and thromboembolism) were recorded and compared.</p><p><strong>Results: </strong>We included 113 eligible patients in the study. The IVIg cohort had a significantly lower initial P/F ratio than the SoC cohort (p=0.01), but the change in P/F ratio was similar (p=0.54). Initial CRP and changes in CRP were similar in the two groups (p=0.38 and p=0.75, respectively), as were initial SOFA score and changes in SOFA score (p=0.18 and p=0.08, respectively) and vasopressor dose on day 0 and day 5 (p=0.97 and p=0.93, respectively). Duration of mechanical ventilation did not differ significantly between the IVIg group and the SoC group (p=0.13). There were no significant differences in measured complications between the two groups. On univariate analysis, the relative risk of death was 1.6 times higher (95% confidence interval (CI) 1.1 - 2.3) in the IVIg group; however, a logistical regression model demonstrated that only a higher P/F ratio (odds ratio (OR) 0.991; 95% CI 0.983 - 0.997) and higher mean airway pressure (OR 1.283; 95% CI 1.026 - 1.604) were significantly associated with ICU mortality.</p><p><strong>Conclusion: </strong>Use of IVIg in our study was directed at an older population, with significantly worse oxygenation. We found no evidence of adverse effects of immunoglobulin therapy; however, we found no benefit either. Only the P/F ratio and mean airway pressure independently predicted ICU mortality.</p><p><strong>Contribution of the study: </strong>During the COVID-19 pandemic, treatment protocols changed in response to the evolving literature. Hospitals were faced with choosing a treatment modality that they believed at the time had benefit. Chris Hani Baragwanath Hospital in Johannesburg, South Africa (SA), incorporated IVIg into its treatment protocols for patients with severe COVID pneumonia requiring ICU admission. This study retrospectively analysed the use of IVIg therapy in the hope of creating a more robust understanding of its safety and efficacy as a treatment option for SA patients in the future.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\"40 3\",\"pages\":\"e1897\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-11-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11792588/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2024.v40i3.1897\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2024.v40i3.1897","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:COVID-19感染具有不同的临床表现,一小部分患者发展为严重疾病,需要重症监护和机械通气,死亡率增加。南非经历了这种大流行的多波,跨越了疫苗接种前和疫苗接种期。治疗的方法和开始是一个有争议的话题,根据不断发展的研究和文献而变化。本研究探讨了高剂量静脉注射免疫球蛋白(IVIg)作为初始药物治疗失败后的补救性治疗。目的:比较重症COVID-19肺炎患者接受IVIg治疗与接受标准护理(SoC)患者在炎症、器官功能障碍和氧合方面的疾病进展。方法:这是一项单中心、回顾性研究,研究对象是南非约翰内斯堡Chris Hani Baragwanath学术医院在疫苗接种前COVID-19大流行期间入住重症监护病房(ICU)的患者。统计数据、炎症标志物(c反应蛋白(CRP))、器官功能(顺序器官衰竭评估(SOFA)评分)、氧合(动脉血氧分压与吸气氧分数之比(P/F比))、总死亡率和并发症(医院感染和血栓栓塞)进行记录和比较。结果:我们纳入了113例符合条件的患者。IVIg组的初始P/F比显著低于SoC组(P =0.01),但P/F比的变化相似(P =0.54)。两组患者的初始CRP和CRP变化相似(p=0.38和p=0.75),初始SOFA评分和SOFA评分变化相似(p=0.18和p=0.08),第0天和第5天的血管加压剂剂量相似(p=0.97和p=0.93)。IVIg组与SoC组机械通气时间无显著差异(p=0.13)。两组间测量的并发症无显著差异。单因素分析显示,IVIg组的相对死亡风险高出1.6倍(95%可信区间(CI) 1.1 - 2.3);然而,逻辑回归模型显示,只有较高的市盈率(优势比(OR) 0.991;95% CI 0.983 - 0.997)和较高的平均气道压(OR 1.283;95% CI 1.026 ~ 1.604)与ICU死亡率显著相关。结论:在我们的研究中,IVIg的使用针对的是氧合明显较差的老年人群。我们没有发现免疫球蛋白治疗不良反应的证据;然而,我们也没有发现任何好处。只有P/F比和平均气道压力独立预测ICU死亡率。研究贡献:在COVID-19大流行期间,治疗方案随着文献的发展而改变。医院面临着选择一种他们当时认为有益的治疗方式的问题。南非约翰内斯堡的克里斯·哈尼·巴拉格瓦纳特医院将IVIg纳入了需要入住ICU的重症COVID - 19肺炎患者的治疗方案。本研究回顾性分析了IVIg治疗的使用情况,希望对其作为未来SA患者的治疗选择的安全性和有效性有更深入的了解。
Use of intravenous immunoglobulin for the treatment of severe COVID-19 in the Chris Hani Baragwanath Academic Hospital intensive care unit, Johannesburg, South Africa.
Background: COVID-19 infection has a variable clinical presentation, with a small subgroup of patients developing severe disease, requiring intensive care with mechanical ventilation, with an increased mortality rate. South Africa (SA) has experienced multiple waves of this pandemic, spanning the pre-vaccine and vaccine periods. The method and initiation of treatment is a debated topic, changing according to evolving research and the literature. The present study investigated the use of high-dose intravenous immunoglobulin (IVIg) as a salvage therapy after initial medical treatment failure.
Objectives: To compare disease progression among critically ill COVID-19 pneumonia patients receiving IVIg therapy with that in patients receiving standard of care (SoC), in respect of inflammation, organ dysfunction and oxygenation.
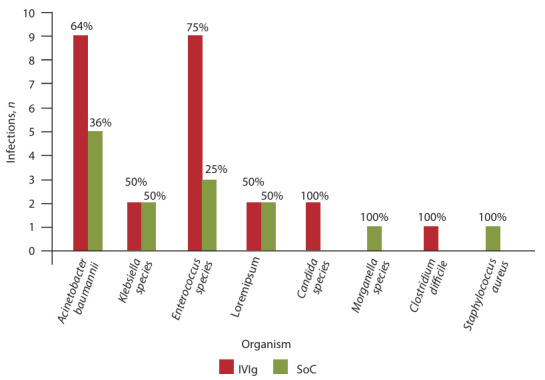
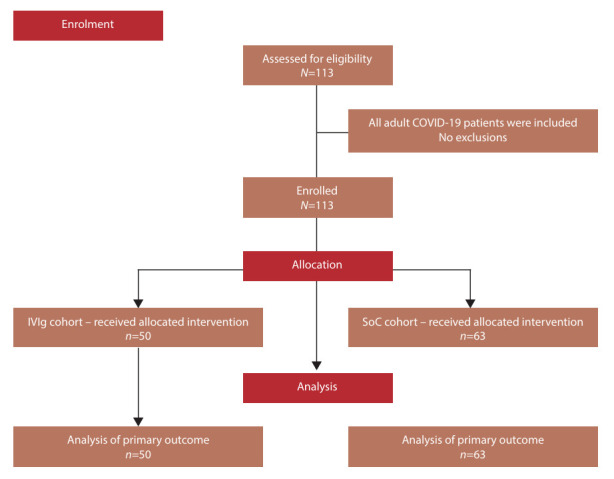
Methods: This was a single-centre, retrospective study of patients admitted to the intensive care unit (ICU) at Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, during the pre-vaccine COVID-19 pandemic. Demographics, inflammatory markers (C-reactive protein (CRP)), organ function (Sequential Organ Failure Assessment (SOFA) score), oxygenation (ratio of partial pressure of oxygen in arterial blood to fraction of inspiratory oxygen (P/F ratio)), overall mortality and complications (nosocomial infections and thromboembolism) were recorded and compared.
Results: We included 113 eligible patients in the study. The IVIg cohort had a significantly lower initial P/F ratio than the SoC cohort (p=0.01), but the change in P/F ratio was similar (p=0.54). Initial CRP and changes in CRP were similar in the two groups (p=0.38 and p=0.75, respectively), as were initial SOFA score and changes in SOFA score (p=0.18 and p=0.08, respectively) and vasopressor dose on day 0 and day 5 (p=0.97 and p=0.93, respectively). Duration of mechanical ventilation did not differ significantly between the IVIg group and the SoC group (p=0.13). There were no significant differences in measured complications between the two groups. On univariate analysis, the relative risk of death was 1.6 times higher (95% confidence interval (CI) 1.1 - 2.3) in the IVIg group; however, a logistical regression model demonstrated that only a higher P/F ratio (odds ratio (OR) 0.991; 95% CI 0.983 - 0.997) and higher mean airway pressure (OR 1.283; 95% CI 1.026 - 1.604) were significantly associated with ICU mortality.
Conclusion: Use of IVIg in our study was directed at an older population, with significantly worse oxygenation. We found no evidence of adverse effects of immunoglobulin therapy; however, we found no benefit either. Only the P/F ratio and mean airway pressure independently predicted ICU mortality.
Contribution of the study: During the COVID-19 pandemic, treatment protocols changed in response to the evolving literature. Hospitals were faced with choosing a treatment modality that they believed at the time had benefit. Chris Hani Baragwanath Hospital in Johannesburg, South Africa (SA), incorporated IVIg into its treatment protocols for patients with severe COVID pneumonia requiring ICU admission. This study retrospectively analysed the use of IVIg therapy in the hope of creating a more robust understanding of its safety and efficacy as a treatment option for SA patients in the future.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


