{"title":"同时使用SGLT2抑制剂治疗住院接受大剂量皮质类固醇治疗的2型糖尿病患者:减轻医源性高血糖","authors":"Kaori Ikeda MD, Fumika Mano-Usui MD, Yo Kishimoto MD, Daisuke Yabe MD, Nobuya Inagaki MD, Koichi Omori MD, Yoji Nagai MD","doi":"10.1111/dom.16221","DOIUrl":null,"url":null,"abstract":"<p>High-dose corticosteroid therapy is vital for anti-inflammation or immunosuppression in certain diseases but often causes hyperglycaemia, treated with insulin injections.<span><sup>1</sup></span> Steroid-induced hyperglycaemia can result from both high-dose and consistent low- to intermediate-dose corticosteroids. Approximately 10%–15% of hospitalised patients consistently use corticosteroids, leading to hyperglycaemia in 56%–86% of individuals, regardless of preexisting diabetes.<span><sup>1</sup></span> Insulin is the recommended treatment for this hyperglycaemia.<span><sup>1</sup></span> Given that sodium-glucose cotransporter 2 inhibitors (SGLT2i) added to insulin therapy typically lower glycaemia and reduce insulin requirements in patients with diabetes,<span><sup>2, 3</sup></span> we hypothesised that SGLT2i could mitigate hyperglycaemia induced by high-dose corticosteroid therapy in individuals with diabetes. Consequently, we investigated the effects of SGLT2i on hyperglycaemia caused by high-dose intravenous corticosteroid pulse treatment in patients with type 2 diabetes.</p><p>We retrospectively collected electronic medical records of patients with type 2 diabetes hospitalised at Kyoto University Hospital between April 2014 and March 2022 who received high-dose corticosteroid therapy for facial paralysis or idiopathic sudden sensorineural hearing loss. These patients received intravenous corticosteroid therapy with 200 mg prednisolone sodium succinate daily for 3 days, followed by 100 mg daily for 3 days, and 50 mg daily for another 3 days. Older patients received a half-dose. Preprandial blood glucose levels were measured using point-of-care (POC) testing devices (PocketChem BG, Arkray, Kyoto, Japan). Data on additional insulin doses used during steroid therapy were also collected. The study was approved by Kyoto University Graduate School and Faculty of Medicine Ethics Committee (R2305-3).</p><p>Eligible patients were identified from medical records using the medical information unit's sorting system. The criteria were as follows: (1) primary diagnosis of facial paralysis or idiopathic sudden sensorineural hearing loss, (2) comorbid diagnosis of type 2 diabetes, (3) intravenous prednisolone sodium succinate administration and (4) POC capillary (finger-stick) glucose monitoring records measured by healthcare professionals in hospitals. Exclusion criteria included (1) early discharge before the third prednisolone dose and (2) incomplete records of three daily preprandial blood glucose measurements in the hospital.</p><p>Demographic and clinical information, including medications, anthropometric data, and HbA1c and preprandial blood glucose levels, were systematically collected from medical records. HbA1c levels were measured before or shortly after admission. The impact of SGLT2i on mean preprandial blood glucose levels during the 7-day hospital stay (pre-breakfast, pre-lunch and pre-dinner levels from day 2 to day 8) was assessed using multiple linear regression analyses. The effects on add-on insulin administered during the 8-day hospital stay (days 1 to 8) under high-dose corticosteroid therapy were also analysed. Statistical significance was set at <i>p</i> <0.05. JMP Pro®, version 16.2.0 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.</p><p>From April 2014 to March 2022, data on 46 patients with type 2 diabetes hospitalised for a 9-day course of high-dose intravenous corticosteroids for facial paralysis or idiopathic sudden sensorineural hearing loss were extracted from electronic medical records. Three were excluded due to early discharge, three for incomplete POC blood glucose monitoring, and one for 15 repeated hypoglycaemic episodes, leaving 39 patients for analysis (Figure S1). The mean age was 63.5 years with a standard deviation of 11.7 years, BMI was 26.0 ± 4.4 kg/m<sup>2</sup>, HbA1c was 7.4% ± 1.7% (57 mmol/mol), preprandial blood glucose level during prednisolone therapy was 189.6 ± 52.2 mg/dL, and the total additional insulin dose required was 62.8 ± 60.9 units per hospital stay. The concurrent use of medications and patient characteristics are shown in Table 1, stratified by SGLT2 inhibitor use (Table 1).</p><p>From potential confounders—age, sex, BMI, HbA1c and prednisolone dose—only HbA1c and age were significant determinants of preprandial blood glucose levels by stepwise regression. For the add-on insulin required for glycaemic control during corticosteroid therapy, HbA1c and pre-therapy insulin dose emerged as significant determinants from the same set of confounders. HbA1c and age were used to adjust the regression model of preprandial blood glucose levels, while HbA1c and pre-therapy insulin dose were used in the regression analysis of insulin dosage.</p><p>In contrast to other medications, concurrent SGLT2i use significantly influenced lower mean preprandial blood glucose levels compared with non-use after adjusting for HbA1c and age (<i>B</i> = −31.8, <i>p</i> = 0.048) (Figure 1). Other medications, including DPP4i (<i>B</i> = 5.9, <i>p</i> = 0.632), metformin (<i>B</i> = −17.1, <i>p</i> = 0.170), sulfonylureas (<i>B</i> = 20.0, <i>p</i> = 0.187), α-glucosidase inhibitors (<i>B</i> = −18.2, <i>p</i> = 0.325) and meglitinides (<i>B</i> = −21.0, <i>p</i> = 0.316), did not show a significant influence on preprandial blood glucose levels. Although not statistically significant, concurrent SGLT2i use tended to reduce the additional insulin dose needed to manage glycaemia during corticosteroid therapy after adjusting for HbA1c and pre-corticosteroid insulin doses (<i>B</i> = −34.8, <i>p</i> = 0.060), a trend not observed with other hypoglycaemic medications, including DPP4i (<i>B</i> = 8.6, <i>p</i> = 0.538), metformin (<i>B</i> = −15.4, <i>p</i> = 0.282), sulfonylureas (<i>B</i> = 6.3, <i>p</i> = 0.720), α-glucosidase inhibitors (<i>B</i> = −23.9, <i>p</i> = 0.257) and meglitinides (<i>B</i> = −22.9, <i>p</i> = 0.334). (Figure S2). No adverse events, such as ketosis or urinary tract infection, were reported.</p><p>SGLT2i was the only medication, besides insulin, significantly linked to decreased hyperglycaemia during corticosteroid therapy, requiring a relatively low add-on insulin dose in this observational study. This result is likely due to an insulin-independent effect on the renal glucose threshold. SGLT2i is known to decrease glycaemic excursions,<span><sup>4, 5</sup></span> and this effect is more pronounced than that of metformin or gliclazide.<span><sup>6, 7</sup></span> Steroid-induced glucose excursions may be effectively targeted by SGLT2i.</p><p>Steroid-induced hyperglycaemia has a poor prognosis.<span><sup>8</sup></span> In hospitals, over half of patients on high-dose steroids develop hyperglycaemia,<span><sup>9</sup></span> typically managed with insulin injections. Optimal corticosteroid regimens for facial paralysis have been established,<span><sup>10, 11</sup></span> and systemic corticosteroid therapy for idiopathic sudden sensorineural hearing loss is common in Japan and optional in America.<span><sup>12, 13</sup></span> Blood glucose increases and insulin dose requirements vary among patients; therefore, insulin adjustments are based on the anticipated dose and duration of glucocorticoid treatment and subsequent glycaemia levels.<span><sup>1</sup></span> Daily insulin adjustments require careful management to avoid hypo- or hyperglycaemia.</p><p>Glucocorticoids act as counter-regulatory hormones to insulin. Elevated glucocorticoid levels combined with dehydration predispose individuals to ketosis.<span><sup>14</sup></span> While no patients in this study showed ketosis symptoms, the risk associated with SGLT2i use under high-dose corticosteroid therapy remains. In hospitalised patients, dehydration can be managed by monitoring and treatment. Patients with facial paralysis or idiopathic sudden sensorineural hearing loss typically maintain good general health, presenting no clear contraindications for SGLT2i.</p><p>Individuals with diabetes treated with SGLT2i exhibit reduced hyperglycaemia during high-dose steroid therapy. The potential benefits of continuing SGLT2i in the setting of steroid administration should not be overlooked. However, limitations include the observational design, small sample size, few patients using GLP-1 receptor agonists, and none using GIP/GLP-1 receptor agonist or imeglimin. Further research is needed to confirm the benefits of SGLT2i in patients with diabetes hospitalised for high-dose corticosteroid therapy.</p><p>KI conceived the research concept. KI, FMU and YK designed the study. KI and FMU collected data. KI, FMU, YK, DY, NI, KO and YN analysed and interpreted the data. KI wrote the manuscript. All authors reviewed the manuscript. KI had full access to all data and ensured data integrity and accuracy of the analysis.</p><p>KI received research funds from Japan Association for Diabetes Education and Care and speaker honoraria from Sanofi, Sumitomo Pharma and Kowa Pharmaceutical. YK received research funds from Kaigen Pharma, Takeda Science Foundation and Smoking Research Foundation and speaker honoraria from Eisai, Meiji Seika Pharma and Merck Biopharma. DY received clinical commissioned or joint research grants from Nippon Boehringer Ingelheim, Eli Lilly Japan, Mitsubishi Tanabe Pharma, MSD and Taisho Pharmaceutical; scholarship grants from ARKRAY, Novo Nordisk Pharma and Taisho Pharmaceutical; and speaker honoraria from Novo Nordisk Pharma, MSD, Eli Lilly Japan and Mitsubishi Tanabe Pharma. NI received clinical commissioned or joint research grants from Terumo, Drawbridge Health and Asken; speaker honoraria from Novo Nordisk, Sumitomo Pharma, Eli Lilly Japan, Sanofi, Kyowa Kirin, Mitsubishi Tanabe Pharma and Nippon Boehringer Ingelheim and scholarship grants from Sumitomo Pharma, Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Takeda Pharmaceutical, Daiichi Sankyo, Kyowa Kirin, MSD, Ono Pharmaceutical, Kowa Pharmaceutical and Lifescan Japan.</p>","PeriodicalId":158,"journal":{"name":"Diabetes, Obesity & Metabolism","volume":"27 4","pages":"2305-2308"},"PeriodicalIF":5.7000,"publicationDate":"2025-02-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dom.16221","citationCount":"0","resultStr":"{\"title\":\"Concurrent SGLT2 inhibitor use in patients with type 2 diabetes hospitalised for high-dose corticosteroid therapy: Mitigated iatrogenic hyperglycaemia\",\"authors\":\"Kaori Ikeda MD, Fumika Mano-Usui MD, Yo Kishimoto MD, Daisuke Yabe MD, Nobuya Inagaki MD, Koichi Omori MD, Yoji Nagai MD\",\"doi\":\"10.1111/dom.16221\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>High-dose corticosteroid therapy is vital for anti-inflammation or immunosuppression in certain diseases but often causes hyperglycaemia, treated with insulin injections.<span><sup>1</sup></span> Steroid-induced hyperglycaemia can result from both high-dose and consistent low- to intermediate-dose corticosteroids. Approximately 10%–15% of hospitalised patients consistently use corticosteroids, leading to hyperglycaemia in 56%–86% of individuals, regardless of preexisting diabetes.<span><sup>1</sup></span> Insulin is the recommended treatment for this hyperglycaemia.<span><sup>1</sup></span> Given that sodium-glucose cotransporter 2 inhibitors (SGLT2i) added to insulin therapy typically lower glycaemia and reduce insulin requirements in patients with diabetes,<span><sup>2, 3</sup></span> we hypothesised that SGLT2i could mitigate hyperglycaemia induced by high-dose corticosteroid therapy in individuals with diabetes. Consequently, we investigated the effects of SGLT2i on hyperglycaemia caused by high-dose intravenous corticosteroid pulse treatment in patients with type 2 diabetes.</p><p>We retrospectively collected electronic medical records of patients with type 2 diabetes hospitalised at Kyoto University Hospital between April 2014 and March 2022 who received high-dose corticosteroid therapy for facial paralysis or idiopathic sudden sensorineural hearing loss. These patients received intravenous corticosteroid therapy with 200 mg prednisolone sodium succinate daily for 3 days, followed by 100 mg daily for 3 days, and 50 mg daily for another 3 days. Older patients received a half-dose. Preprandial blood glucose levels were measured using point-of-care (POC) testing devices (PocketChem BG, Arkray, Kyoto, Japan). Data on additional insulin doses used during steroid therapy were also collected. The study was approved by Kyoto University Graduate School and Faculty of Medicine Ethics Committee (R2305-3).</p><p>Eligible patients were identified from medical records using the medical information unit's sorting system. The criteria were as follows: (1) primary diagnosis of facial paralysis or idiopathic sudden sensorineural hearing loss, (2) comorbid diagnosis of type 2 diabetes, (3) intravenous prednisolone sodium succinate administration and (4) POC capillary (finger-stick) glucose monitoring records measured by healthcare professionals in hospitals. Exclusion criteria included (1) early discharge before the third prednisolone dose and (2) incomplete records of three daily preprandial blood glucose measurements in the hospital.</p><p>Demographic and clinical information, including medications, anthropometric data, and HbA1c and preprandial blood glucose levels, were systematically collected from medical records. HbA1c levels were measured before or shortly after admission. The impact of SGLT2i on mean preprandial blood glucose levels during the 7-day hospital stay (pre-breakfast, pre-lunch and pre-dinner levels from day 2 to day 8) was assessed using multiple linear regression analyses. The effects on add-on insulin administered during the 8-day hospital stay (days 1 to 8) under high-dose corticosteroid therapy were also analysed. Statistical significance was set at <i>p</i> <0.05. JMP Pro®, version 16.2.0 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.</p><p>From April 2014 to March 2022, data on 46 patients with type 2 diabetes hospitalised for a 9-day course of high-dose intravenous corticosteroids for facial paralysis or idiopathic sudden sensorineural hearing loss were extracted from electronic medical records. Three were excluded due to early discharge, three for incomplete POC blood glucose monitoring, and one for 15 repeated hypoglycaemic episodes, leaving 39 patients for analysis (Figure S1). The mean age was 63.5 years with a standard deviation of 11.7 years, BMI was 26.0 ± 4.4 kg/m<sup>2</sup>, HbA1c was 7.4% ± 1.7% (57 mmol/mol), preprandial blood glucose level during prednisolone therapy was 189.6 ± 52.2 mg/dL, and the total additional insulin dose required was 62.8 ± 60.9 units per hospital stay. The concurrent use of medications and patient characteristics are shown in Table 1, stratified by SGLT2 inhibitor use (Table 1).</p><p>From potential confounders—age, sex, BMI, HbA1c and prednisolone dose—only HbA1c and age were significant determinants of preprandial blood glucose levels by stepwise regression. For the add-on insulin required for glycaemic control during corticosteroid therapy, HbA1c and pre-therapy insulin dose emerged as significant determinants from the same set of confounders. HbA1c and age were used to adjust the regression model of preprandial blood glucose levels, while HbA1c and pre-therapy insulin dose were used in the regression analysis of insulin dosage.</p><p>In contrast to other medications, concurrent SGLT2i use significantly influenced lower mean preprandial blood glucose levels compared with non-use after adjusting for HbA1c and age (<i>B</i> = −31.8, <i>p</i> = 0.048) (Figure 1). Other medications, including DPP4i (<i>B</i> = 5.9, <i>p</i> = 0.632), metformin (<i>B</i> = −17.1, <i>p</i> = 0.170), sulfonylureas (<i>B</i> = 20.0, <i>p</i> = 0.187), α-glucosidase inhibitors (<i>B</i> = −18.2, <i>p</i> = 0.325) and meglitinides (<i>B</i> = −21.0, <i>p</i> = 0.316), did not show a significant influence on preprandial blood glucose levels. Although not statistically significant, concurrent SGLT2i use tended to reduce the additional insulin dose needed to manage glycaemia during corticosteroid therapy after adjusting for HbA1c and pre-corticosteroid insulin doses (<i>B</i> = −34.8, <i>p</i> = 0.060), a trend not observed with other hypoglycaemic medications, including DPP4i (<i>B</i> = 8.6, <i>p</i> = 0.538), metformin (<i>B</i> = −15.4, <i>p</i> = 0.282), sulfonylureas (<i>B</i> = 6.3, <i>p</i> = 0.720), α-glucosidase inhibitors (<i>B</i> = −23.9, <i>p</i> = 0.257) and meglitinides (<i>B</i> = −22.9, <i>p</i> = 0.334). (Figure S2). No adverse events, such as ketosis or urinary tract infection, were reported.</p><p>SGLT2i was the only medication, besides insulin, significantly linked to decreased hyperglycaemia during corticosteroid therapy, requiring a relatively low add-on insulin dose in this observational study. This result is likely due to an insulin-independent effect on the renal glucose threshold. SGLT2i is known to decrease glycaemic excursions,<span><sup>4, 5</sup></span> and this effect is more pronounced than that of metformin or gliclazide.<span><sup>6, 7</sup></span> Steroid-induced glucose excursions may be effectively targeted by SGLT2i.</p><p>Steroid-induced hyperglycaemia has a poor prognosis.<span><sup>8</sup></span> In hospitals, over half of patients on high-dose steroids develop hyperglycaemia,<span><sup>9</sup></span> typically managed with insulin injections. Optimal corticosteroid regimens for facial paralysis have been established,<span><sup>10, 11</sup></span> and systemic corticosteroid therapy for idiopathic sudden sensorineural hearing loss is common in Japan and optional in America.<span><sup>12, 13</sup></span> Blood glucose increases and insulin dose requirements vary among patients; therefore, insulin adjustments are based on the anticipated dose and duration of glucocorticoid treatment and subsequent glycaemia levels.<span><sup>1</sup></span> Daily insulin adjustments require careful management to avoid hypo- or hyperglycaemia.</p><p>Glucocorticoids act as counter-regulatory hormones to insulin. Elevated glucocorticoid levels combined with dehydration predispose individuals to ketosis.<span><sup>14</sup></span> While no patients in this study showed ketosis symptoms, the risk associated with SGLT2i use under high-dose corticosteroid therapy remains. In hospitalised patients, dehydration can be managed by monitoring and treatment. Patients with facial paralysis or idiopathic sudden sensorineural hearing loss typically maintain good general health, presenting no clear contraindications for SGLT2i.</p><p>Individuals with diabetes treated with SGLT2i exhibit reduced hyperglycaemia during high-dose steroid therapy. The potential benefits of continuing SGLT2i in the setting of steroid administration should not be overlooked. However, limitations include the observational design, small sample size, few patients using GLP-1 receptor agonists, and none using GIP/GLP-1 receptor agonist or imeglimin. Further research is needed to confirm the benefits of SGLT2i in patients with diabetes hospitalised for high-dose corticosteroid therapy.</p><p>KI conceived the research concept. KI, FMU and YK designed the study. KI and FMU collected data. KI, FMU, YK, DY, NI, KO and YN analysed and interpreted the data. KI wrote the manuscript. All authors reviewed the manuscript. KI had full access to all data and ensured data integrity and accuracy of the analysis.</p><p>KI received research funds from Japan Association for Diabetes Education and Care and speaker honoraria from Sanofi, Sumitomo Pharma and Kowa Pharmaceutical. YK received research funds from Kaigen Pharma, Takeda Science Foundation and Smoking Research Foundation and speaker honoraria from Eisai, Meiji Seika Pharma and Merck Biopharma. DY received clinical commissioned or joint research grants from Nippon Boehringer Ingelheim, Eli Lilly Japan, Mitsubishi Tanabe Pharma, MSD and Taisho Pharmaceutical; scholarship grants from ARKRAY, Novo Nordisk Pharma and Taisho Pharmaceutical; and speaker honoraria from Novo Nordisk Pharma, MSD, Eli Lilly Japan and Mitsubishi Tanabe Pharma. NI received clinical commissioned or joint research grants from Terumo, Drawbridge Health and Asken; speaker honoraria from Novo Nordisk, Sumitomo Pharma, Eli Lilly Japan, Sanofi, Kyowa Kirin, Mitsubishi Tanabe Pharma and Nippon Boehringer Ingelheim and scholarship grants from Sumitomo Pharma, Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Takeda Pharmaceutical, Daiichi Sankyo, Kyowa Kirin, MSD, Ono Pharmaceutical, Kowa Pharmaceutical and Lifescan Japan.</p>\",\"PeriodicalId\":158,\"journal\":{\"name\":\"Diabetes, Obesity & Metabolism\",\"volume\":\"27 4\",\"pages\":\"2305-2308\"},\"PeriodicalIF\":5.7000,\"publicationDate\":\"2025-02-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/dom.16221\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes, Obesity & Metabolism\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/dom.16221\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes, Obesity & Metabolism","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/dom.16221","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
187)、α-葡萄糖苷酶抑制剂(B = - 18.2, p = 0.325)和美格列汀类药物(B = - 21.0, p = 0.316)对餐前血糖水平没有显著影响。虽然没有统计学意义,并发SGLT2i使用倾向于减少额外的胰岛素剂量皮质类固醇治疗期间需要管理glycaemia调整后糖化血红蛋白和pre-corticosteroid胰岛素剂量(B =−34.8,p = 0.060),这一趋势与其他那些没有观察到药物,包括DPP4i (B = 8.6, p = 0.538),二甲双胍(B =−15.4,p = 0.282),磺酰脲类药物(B = 6.3, p = 0.720),α葡糖苷酶抑制剂(B =−23.9,p = 0.257)和meglitinides (B =−22.9,p = 0.334)。(图S2)。没有不良事件,如酮症或尿路感染的报道。在本观察性研究中,SGLT2i是除胰岛素外唯一与皮质类固醇治疗期间高血糖降低显著相关的药物,需要相对较低的附加胰岛素剂量。这一结果可能是由于胰岛素对肾葡萄糖阈值的非依赖型影响。已知SGLT2i可降低血糖漂移4,5,其效果比二甲双胍或格列齐特更为明显。6,7甾体诱导的葡萄糖漂移可能被SGLT2i有效靶向。类固醇引起的高血糖预后不良在医院里,超过一半服用大剂量类固醇的患者会出现高血糖,9通常通过注射胰岛素来治疗。面瘫的最佳皮质类固醇治疗方案已经建立10,11,特发性突发性感觉神经性听力损失的全身性皮质类固醇治疗在日本很常见,在美国是可选的12,13。因此,胰岛素的调整是基于糖皮质激素治疗的预期剂量和持续时间以及随后的血糖水平每日胰岛素调整需要谨慎管理,以避免低血糖或高血糖。糖皮质激素作为胰岛素的反调节激素。糖皮质激素水平升高加上脱水使个体易患酮症虽然本研究中没有患者出现酮症症状,但在大剂量皮质类固醇治疗下使用SGLT2i的相关风险仍然存在。在住院病人中,可以通过监测和治疗来控制脱水。面瘫或特发性突发性感音神经性听力损失患者通常保持良好的总体健康状况,没有明确的SGLT2i禁忌症。用SGLT2i治疗的糖尿病患者在大剂量类固醇治疗期间表现出高血糖的降低。在类固醇给药的情况下,持续SGLT2i的潜在益处不应被忽视。然而,局限性包括观察性设计,样本量小,很少患者使用GLP-1受体激动剂,并且没有患者使用GIP/GLP-1受体激动剂或伊美霉素。需要进一步的研究来证实SGLT2i对住院接受大剂量皮质类固醇治疗的糖尿病患者的益处。KI提出了研究概念。KI, FMU和YK设计了这项研究。KI和FMU采集数据。KI, FMU, YK, DY, NI, KO和YN分析和解释数据。KI写了手稿。所有作者都审阅了手稿。KI拥有对所有数据的完全访问权,确保了数据的完整性和分析的准确性。KI获得了日本糖尿病教育与护理协会的研究经费,并获得了赛诺菲、住友制药和大和制药的演讲荣誉。YK获得了凯根制药、武田科学基金会和吸烟研究基金会的研究经费,并获得了卫材、明治精华制药和默克生物制药的荣誉演讲。获得Nippon Boehringer Ingelheim, Eli Lilly Japan, Mitsubishi Tanabe Pharma, MSD and Taisho Pharmaceutical的临床委托或联合研究资助;ARKRAY、诺和诺德制药和大正制药的奖学金;以及诺和诺德制药、默沙东、礼来日本和三菱田边制药的荣誉演讲嘉宾。NI获得了Terumo、Drawbridge Health和Asken的临床委托或联合研究资助;来自诺和诺德、住友制药、礼来日本、赛诺菲、协和麒麟、三菱田边制药和日本勃林格殷格翰的荣誉演讲嘉宾,以及住友制药、三菱田边制药、日本勃林格殷格翰、武田制药、第一三共、协和麒麟、默沙东、小野制药、和田制药和日本Lifescan的奖学金。
Concurrent SGLT2 inhibitor use in patients with type 2 diabetes hospitalised for high-dose corticosteroid therapy: Mitigated iatrogenic hyperglycaemia
High-dose corticosteroid therapy is vital for anti-inflammation or immunosuppression in certain diseases but often causes hyperglycaemia, treated with insulin injections.1 Steroid-induced hyperglycaemia can result from both high-dose and consistent low- to intermediate-dose corticosteroids. Approximately 10%–15% of hospitalised patients consistently use corticosteroids, leading to hyperglycaemia in 56%–86% of individuals, regardless of preexisting diabetes.1 Insulin is the recommended treatment for this hyperglycaemia.1 Given that sodium-glucose cotransporter 2 inhibitors (SGLT2i) added to insulin therapy typically lower glycaemia and reduce insulin requirements in patients with diabetes,2, 3 we hypothesised that SGLT2i could mitigate hyperglycaemia induced by high-dose corticosteroid therapy in individuals with diabetes. Consequently, we investigated the effects of SGLT2i on hyperglycaemia caused by high-dose intravenous corticosteroid pulse treatment in patients with type 2 diabetes.
We retrospectively collected electronic medical records of patients with type 2 diabetes hospitalised at Kyoto University Hospital between April 2014 and March 2022 who received high-dose corticosteroid therapy for facial paralysis or idiopathic sudden sensorineural hearing loss. These patients received intravenous corticosteroid therapy with 200 mg prednisolone sodium succinate daily for 3 days, followed by 100 mg daily for 3 days, and 50 mg daily for another 3 days. Older patients received a half-dose. Preprandial blood glucose levels were measured using point-of-care (POC) testing devices (PocketChem BG, Arkray, Kyoto, Japan). Data on additional insulin doses used during steroid therapy were also collected. The study was approved by Kyoto University Graduate School and Faculty of Medicine Ethics Committee (R2305-3).
Eligible patients were identified from medical records using the medical information unit's sorting system. The criteria were as follows: (1) primary diagnosis of facial paralysis or idiopathic sudden sensorineural hearing loss, (2) comorbid diagnosis of type 2 diabetes, (3) intravenous prednisolone sodium succinate administration and (4) POC capillary (finger-stick) glucose monitoring records measured by healthcare professionals in hospitals. Exclusion criteria included (1) early discharge before the third prednisolone dose and (2) incomplete records of three daily preprandial blood glucose measurements in the hospital.
Demographic and clinical information, including medications, anthropometric data, and HbA1c and preprandial blood glucose levels, were systematically collected from medical records. HbA1c levels were measured before or shortly after admission. The impact of SGLT2i on mean preprandial blood glucose levels during the 7-day hospital stay (pre-breakfast, pre-lunch and pre-dinner levels from day 2 to day 8) was assessed using multiple linear regression analyses. The effects on add-on insulin administered during the 8-day hospital stay (days 1 to 8) under high-dose corticosteroid therapy were also analysed. Statistical significance was set at p <0.05. JMP Pro®, version 16.2.0 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.
From April 2014 to March 2022, data on 46 patients with type 2 diabetes hospitalised for a 9-day course of high-dose intravenous corticosteroids for facial paralysis or idiopathic sudden sensorineural hearing loss were extracted from electronic medical records. Three were excluded due to early discharge, three for incomplete POC blood glucose monitoring, and one for 15 repeated hypoglycaemic episodes, leaving 39 patients for analysis (Figure S1). The mean age was 63.5 years with a standard deviation of 11.7 years, BMI was 26.0 ± 4.4 kg/m2, HbA1c was 7.4% ± 1.7% (57 mmol/mol), preprandial blood glucose level during prednisolone therapy was 189.6 ± 52.2 mg/dL, and the total additional insulin dose required was 62.8 ± 60.9 units per hospital stay. The concurrent use of medications and patient characteristics are shown in Table 1, stratified by SGLT2 inhibitor use (Table 1).
From potential confounders—age, sex, BMI, HbA1c and prednisolone dose—only HbA1c and age were significant determinants of preprandial blood glucose levels by stepwise regression. For the add-on insulin required for glycaemic control during corticosteroid therapy, HbA1c and pre-therapy insulin dose emerged as significant determinants from the same set of confounders. HbA1c and age were used to adjust the regression model of preprandial blood glucose levels, while HbA1c and pre-therapy insulin dose were used in the regression analysis of insulin dosage.
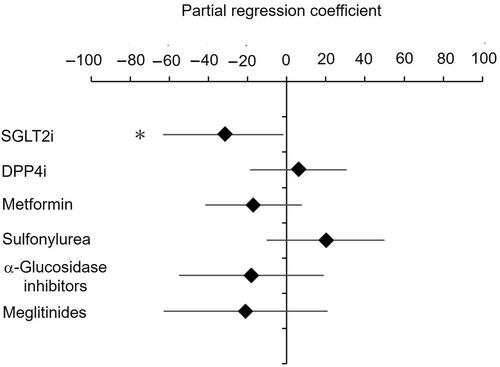
In contrast to other medications, concurrent SGLT2i use significantly influenced lower mean preprandial blood glucose levels compared with non-use after adjusting for HbA1c and age (B = −31.8, p = 0.048) (Figure 1). Other medications, including DPP4i (B = 5.9, p = 0.632), metformin (B = −17.1, p = 0.170), sulfonylureas (B = 20.0, p = 0.187), α-glucosidase inhibitors (B = −18.2, p = 0.325) and meglitinides (B = −21.0, p = 0.316), did not show a significant influence on preprandial blood glucose levels. Although not statistically significant, concurrent SGLT2i use tended to reduce the additional insulin dose needed to manage glycaemia during corticosteroid therapy after adjusting for HbA1c and pre-corticosteroid insulin doses (B = −34.8, p = 0.060), a trend not observed with other hypoglycaemic medications, including DPP4i (B = 8.6, p = 0.538), metformin (B = −15.4, p = 0.282), sulfonylureas (B = 6.3, p = 0.720), α-glucosidase inhibitors (B = −23.9, p = 0.257) and meglitinides (B = −22.9, p = 0.334). (Figure S2). No adverse events, such as ketosis or urinary tract infection, were reported.
SGLT2i was the only medication, besides insulin, significantly linked to decreased hyperglycaemia during corticosteroid therapy, requiring a relatively low add-on insulin dose in this observational study. This result is likely due to an insulin-independent effect on the renal glucose threshold. SGLT2i is known to decrease glycaemic excursions,4, 5 and this effect is more pronounced than that of metformin or gliclazide.6, 7 Steroid-induced glucose excursions may be effectively targeted by SGLT2i.
Steroid-induced hyperglycaemia has a poor prognosis.8 In hospitals, over half of patients on high-dose steroids develop hyperglycaemia,9 typically managed with insulin injections. Optimal corticosteroid regimens for facial paralysis have been established,10, 11 and systemic corticosteroid therapy for idiopathic sudden sensorineural hearing loss is common in Japan and optional in America.12, 13 Blood glucose increases and insulin dose requirements vary among patients; therefore, insulin adjustments are based on the anticipated dose and duration of glucocorticoid treatment and subsequent glycaemia levels.1 Daily insulin adjustments require careful management to avoid hypo- or hyperglycaemia.
Glucocorticoids act as counter-regulatory hormones to insulin. Elevated glucocorticoid levels combined with dehydration predispose individuals to ketosis.14 While no patients in this study showed ketosis symptoms, the risk associated with SGLT2i use under high-dose corticosteroid therapy remains. In hospitalised patients, dehydration can be managed by monitoring and treatment. Patients with facial paralysis or idiopathic sudden sensorineural hearing loss typically maintain good general health, presenting no clear contraindications for SGLT2i.
Individuals with diabetes treated with SGLT2i exhibit reduced hyperglycaemia during high-dose steroid therapy. The potential benefits of continuing SGLT2i in the setting of steroid administration should not be overlooked. However, limitations include the observational design, small sample size, few patients using GLP-1 receptor agonists, and none using GIP/GLP-1 receptor agonist or imeglimin. Further research is needed to confirm the benefits of SGLT2i in patients with diabetes hospitalised for high-dose corticosteroid therapy.
KI conceived the research concept. KI, FMU and YK designed the study. KI and FMU collected data. KI, FMU, YK, DY, NI, KO and YN analysed and interpreted the data. KI wrote the manuscript. All authors reviewed the manuscript. KI had full access to all data and ensured data integrity and accuracy of the analysis.
KI received research funds from Japan Association for Diabetes Education and Care and speaker honoraria from Sanofi, Sumitomo Pharma and Kowa Pharmaceutical. YK received research funds from Kaigen Pharma, Takeda Science Foundation and Smoking Research Foundation and speaker honoraria from Eisai, Meiji Seika Pharma and Merck Biopharma. DY received clinical commissioned or joint research grants from Nippon Boehringer Ingelheim, Eli Lilly Japan, Mitsubishi Tanabe Pharma, MSD and Taisho Pharmaceutical; scholarship grants from ARKRAY, Novo Nordisk Pharma and Taisho Pharmaceutical; and speaker honoraria from Novo Nordisk Pharma, MSD, Eli Lilly Japan and Mitsubishi Tanabe Pharma. NI received clinical commissioned or joint research grants from Terumo, Drawbridge Health and Asken; speaker honoraria from Novo Nordisk, Sumitomo Pharma, Eli Lilly Japan, Sanofi, Kyowa Kirin, Mitsubishi Tanabe Pharma and Nippon Boehringer Ingelheim and scholarship grants from Sumitomo Pharma, Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Takeda Pharmaceutical, Daiichi Sankyo, Kyowa Kirin, MSD, Ono Pharmaceutical, Kowa Pharmaceutical and Lifescan Japan.
期刊介绍:
Diabetes, Obesity and Metabolism is primarily a journal of clinical and experimental pharmacology and therapeutics covering the interrelated areas of diabetes, obesity and metabolism. The journal prioritises high-quality original research that reports on the effects of new or existing therapies, including dietary, exercise and lifestyle (non-pharmacological) interventions, in any aspect of metabolic and endocrine disease, either in humans or animal and cellular systems. ‘Metabolism’ may relate to lipids, bone and drug metabolism, or broader aspects of endocrine dysfunction. Preclinical pharmacology, pharmacokinetic studies, meta-analyses and those addressing drug safety and tolerability are also highly suitable for publication in this journal. Original research may be published as a main paper or as a research letter.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


