Manuel Comabella, Agustín Pappolla, Enric Monreal, Nicolás Fissolo, Augusto Cesaar Sao-Avilés, Georgina Arrambide, Pere Carbonell-Mirabent, Lucía Gutierrez, Álvaro Cobo-Calvo, Carmen Tur, Javier Villacieros-Álvarez, Ángela Vidal-Jordana, Joaquín Castilló, Ingrid Galán, Mercedes Espiño, Helena Ariño, Luca Bollo, Marta Rodríguez Barranco, Luciana Soledad Midaglia, René Carvajal, Noelia Villarrubia, José Ignacio Fernández Velasco, Breogán Rodríguez Acevedo, Lucienne F Costa Frossard, Andreu Vilaseca, Cristina Auger, Ana Zabalza, Susana Sainz De La Maza, Neus Mongay-Ochoa, Jordi Río, Jaume Sastre-Garriga, Àlex Rovira, Mar Tintoré, Luisa M Villar, Xavier Montalban
{"title":"血液生物标志物对多发性硬化诊断的贡献。","authors":"Manuel Comabella, Agustín Pappolla, Enric Monreal, Nicolás Fissolo, Augusto Cesaar Sao-Avilés, Georgina Arrambide, Pere Carbonell-Mirabent, Lucía Gutierrez, Álvaro Cobo-Calvo, Carmen Tur, Javier Villacieros-Álvarez, Ángela Vidal-Jordana, Joaquín Castilló, Ingrid Galán, Mercedes Espiño, Helena Ariño, Luca Bollo, Marta Rodríguez Barranco, Luciana Soledad Midaglia, René Carvajal, Noelia Villarrubia, José Ignacio Fernández Velasco, Breogán Rodríguez Acevedo, Lucienne F Costa Frossard, Andreu Vilaseca, Cristina Auger, Ana Zabalza, Susana Sainz De La Maza, Neus Mongay-Ochoa, Jordi Río, Jaume Sastre-Garriga, Àlex Rovira, Mar Tintoré, Luisa M Villar, Xavier Montalban","doi":"10.1212/NXI.0000000000200370","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Invasive procedures may delay the diagnostic process in multiple sclerosis (MS). We investigated the added value of serum neurofilament light chain (sNfL), glial fibrillary acidic protein (sGFAP), chitinase-3-like 1 (sCHI3L1), and the immune responses to the Epstein-Barr virus-encoded nuclear antigen 1 to current MS diagnostic criteria.</p><p><strong>Methods: </strong>In this multicentric study, we selected patients from 2 prospective cohorts presenting a clinically isolated syndrome (CIS). Patients were classified as (1) not presenting dissemination in space (DIS) nor dissemination in time (DIT) (noDIS and noDIT); (2) presenting DIS without DIT (DIS and noDIT); and (3) presenting both (DIS and DIT), which were used as a reference. sNfL, sGFAP, and sCHI3L1 levels were measured with single-molecule array immunoassays and EBNA1-specific IgG levels with ELISA. Biomarker levels were compared between groups using linear regression models. Receiver operating characteristic curve analyses and Youden Index were used to determine cutoff values associated with MS diagnosis during follow-up.</p><p><strong>Results: </strong>We included 181 patients (66.3% females, mean [SD] age of 35.0 [9.7] years). At baseline, 25 (13.8%) were classified as noDIS and noDIT, 62 (34.3%) as DIS and noDIT, and 94 (51.9%) as DIS and DIT. Only sNfL Z-scores discriminated between groups (DIS and DIT vs DIS and noDIT [<i>p</i> = 0.002], DIS and DIT vs noDIS and noDIT [<i>p</i> < 0.001], and DIS and noDIT vs noDIS and noDIT [<i>p</i> = 0.026]). In noDIS and noDIT patients (median interquartile range [IQR] follow-up of 8.1 [5.0-11.7] years), high sNfL Z-scores best predicted MS diagnosis (specificity [SP] and 95% CI of 93.3% [68.1-99.8] and positive predictive value [PPV] of 87.5% [47.3-99.7]). Among DIS and noDIT patients (median [IQR] follow-up of 6.8 [4.0-9.1] years), high sNfL Z-scores best predicted MS diagnosis (SP of 80% [28.4-99.5] and PPV of 97.3% [85.8-99.9]) without considering oligoclonal band (OB) status. In the subset of patients of this group with negative OBs, a combination of high sNfL Z-scores and sGFAP levels predicted MS diagnosis (SP of 100% [39.8-100] and PPV of 100% [54.1-100]).</p><p><strong>Discussion: </strong>These results suggest that sNfL and sGFAP may be incorporated in particular scenarios to diagnose MS in patients with CIS not fulfilling current diagnostic criteria.</p>","PeriodicalId":19472,"journal":{"name":"Neurology® Neuroimmunology & Neuroinflammation","volume":"12 2","pages":"e200370"},"PeriodicalIF":7.5000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11781269/pdf/","citationCount":"0","resultStr":"{\"title\":\"Contribution of Blood Biomarkers to Multiple Sclerosis Diagnosis.\",\"authors\":\"Manuel Comabella, Agustín Pappolla, Enric Monreal, Nicolás Fissolo, Augusto Cesaar Sao-Avilés, Georgina Arrambide, Pere Carbonell-Mirabent, Lucía Gutierrez, Álvaro Cobo-Calvo, Carmen Tur, Javier Villacieros-Álvarez, Ángela Vidal-Jordana, Joaquín Castilló, Ingrid Galán, Mercedes Espiño, Helena Ariño, Luca Bollo, Marta Rodríguez Barranco, Luciana Soledad Midaglia, René Carvajal, Noelia Villarrubia, José Ignacio Fernández Velasco, Breogán Rodríguez Acevedo, Lucienne F Costa Frossard, Andreu Vilaseca, Cristina Auger, Ana Zabalza, Susana Sainz De La Maza, Neus Mongay-Ochoa, Jordi Río, Jaume Sastre-Garriga, Àlex Rovira, Mar Tintoré, Luisa M Villar, Xavier Montalban\",\"doi\":\"10.1212/NXI.0000000000200370\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Invasive procedures may delay the diagnostic process in multiple sclerosis (MS). We investigated the added value of serum neurofilament light chain (sNfL), glial fibrillary acidic protein (sGFAP), chitinase-3-like 1 (sCHI3L1), and the immune responses to the Epstein-Barr virus-encoded nuclear antigen 1 to current MS diagnostic criteria.</p><p><strong>Methods: </strong>In this multicentric study, we selected patients from 2 prospective cohorts presenting a clinically isolated syndrome (CIS). Patients were classified as (1) not presenting dissemination in space (DIS) nor dissemination in time (DIT) (noDIS and noDIT); (2) presenting DIS without DIT (DIS and noDIT); and (3) presenting both (DIS and DIT), which were used as a reference. sNfL, sGFAP, and sCHI3L1 levels were measured with single-molecule array immunoassays and EBNA1-specific IgG levels with ELISA. Biomarker levels were compared between groups using linear regression models. Receiver operating characteristic curve analyses and Youden Index were used to determine cutoff values associated with MS diagnosis during follow-up.</p><p><strong>Results: </strong>We included 181 patients (66.3% females, mean [SD] age of 35.0 [9.7] years). At baseline, 25 (13.8%) were classified as noDIS and noDIT, 62 (34.3%) as DIS and noDIT, and 94 (51.9%) as DIS and DIT. Only sNfL Z-scores discriminated between groups (DIS and DIT vs DIS and noDIT [<i>p</i> = 0.002], DIS and DIT vs noDIS and noDIT [<i>p</i> < 0.001], and DIS and noDIT vs noDIS and noDIT [<i>p</i> = 0.026]). In noDIS and noDIT patients (median interquartile range [IQR] follow-up of 8.1 [5.0-11.7] years), high sNfL Z-scores best predicted MS diagnosis (specificity [SP] and 95% CI of 93.3% [68.1-99.8] and positive predictive value [PPV] of 87.5% [47.3-99.7]). Among DIS and noDIT patients (median [IQR] follow-up of 6.8 [4.0-9.1] years), high sNfL Z-scores best predicted MS diagnosis (SP of 80% [28.4-99.5] and PPV of 97.3% [85.8-99.9]) without considering oligoclonal band (OB) status. In the subset of patients of this group with negative OBs, a combination of high sNfL Z-scores and sGFAP levels predicted MS diagnosis (SP of 100% [39.8-100] and PPV of 100% [54.1-100]).</p><p><strong>Discussion: </strong>These results suggest that sNfL and sGFAP may be incorporated in particular scenarios to diagnose MS in patients with CIS not fulfilling current diagnostic criteria.</p>\",\"PeriodicalId\":19472,\"journal\":{\"name\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"volume\":\"12 2\",\"pages\":\"e200370\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11781269/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology® Neuroimmunology & Neuroinflammation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1212/NXI.0000000000200370\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology® Neuroimmunology & Neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000200370","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:侵入性手术可能会延迟多发性硬化症(MS)的诊断过程。我们研究了血清神经丝轻链(sNfL)、胶质纤维酸性蛋白(sGFAP)、几丁质酶-3样1 (sCHI3L1)和对Epstein-Barr病毒编码核抗原1的免疫应答对当前MS诊断标准的附加价值。方法:在这项多中心研究中,我们从2个表现为临床孤立综合征(CIS)的前瞻性队列中选择患者。患者分为(1)无空间播散(DIS),无时间播散(DIT) (noDIS和noDIT);(2)无DIT的DIS (DIS和noDIT);(3)同时给出(DIS和DIT),作为参考。用单分子阵列免疫分析法检测sNfL、sGFAP和sCHI3L1水平,用ELISA法检测ebna1特异性IgG水平。采用线性回归模型比较各组生物标志物水平。随访时采用受试者工作特征曲线分析和约登指数确定与多发性硬化症诊断相关的临界值。结果:纳入181例患者(66.3%为女性,平均[SD]年龄35.0[9.7]岁)。基线时,25例(13.8%)为noDIS和noDIT, 62例(34.3%)为DIS和noDIT, 94例(51.9%)为DIS和DIT。只有sNfL z分数在组间有区别(DIS和DIT vs DIS和noDIT [p = 0.002], DIS和DIT vs noDIS和noDIT [p < 0.001], DIS和noDIT vs noDIS和noDIT [p = 0.026])。在noDIS和noDIT患者中(中位四分位数范围[IQR]随访8.1[5.0-11.7]年),高sNfL z -评分最能预测MS的诊断(特异性[SP]和95% CI为93.3%[68.1-99.8],阳性预测值[PPV]为87.5%[47.3-99.7])。在DIS和noDIT患者(中位[IQR]随访时间为6.8年[4.0-9.1]年)中,高sNfL z -评分最能预测MS诊断(SP为80% [28.4-99.5],PPV为97.3%[85.8-99.9]),而无需考虑寡克隆带(OB)状态。在本组OBs阴性的患者亚组中,高sNfL z -score和sGFAP水平的结合可预测MS诊断(SP为100% [39.8-100],PPV为100%[54.1-100])。讨论:这些结果表明,sNfL和sGFAP可能在特定情况下被纳入诊断不符合当前诊断标准的CIS患者的MS。
Contribution of Blood Biomarkers to Multiple Sclerosis Diagnosis.
Background and objectives: Invasive procedures may delay the diagnostic process in multiple sclerosis (MS). We investigated the added value of serum neurofilament light chain (sNfL), glial fibrillary acidic protein (sGFAP), chitinase-3-like 1 (sCHI3L1), and the immune responses to the Epstein-Barr virus-encoded nuclear antigen 1 to current MS diagnostic criteria.
Methods: In this multicentric study, we selected patients from 2 prospective cohorts presenting a clinically isolated syndrome (CIS). Patients were classified as (1) not presenting dissemination in space (DIS) nor dissemination in time (DIT) (noDIS and noDIT); (2) presenting DIS without DIT (DIS and noDIT); and (3) presenting both (DIS and DIT), which were used as a reference. sNfL, sGFAP, and sCHI3L1 levels were measured with single-molecule array immunoassays and EBNA1-specific IgG levels with ELISA. Biomarker levels were compared between groups using linear regression models. Receiver operating characteristic curve analyses and Youden Index were used to determine cutoff values associated with MS diagnosis during follow-up.
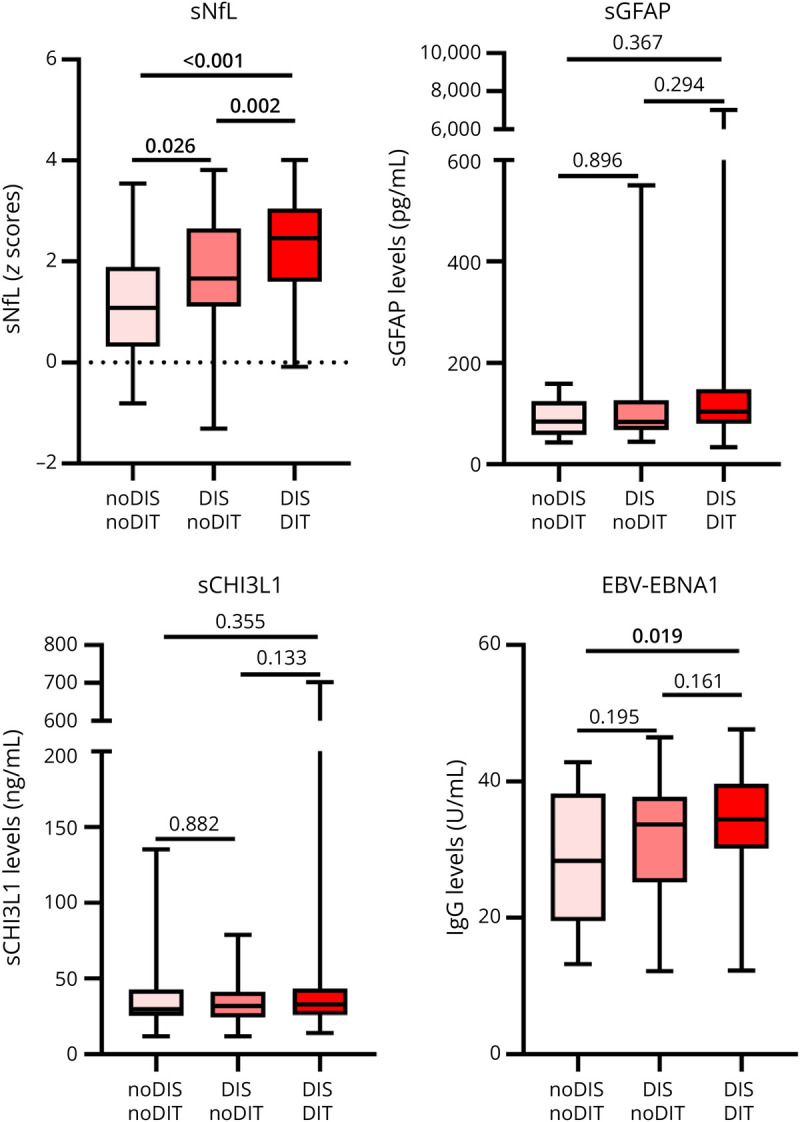
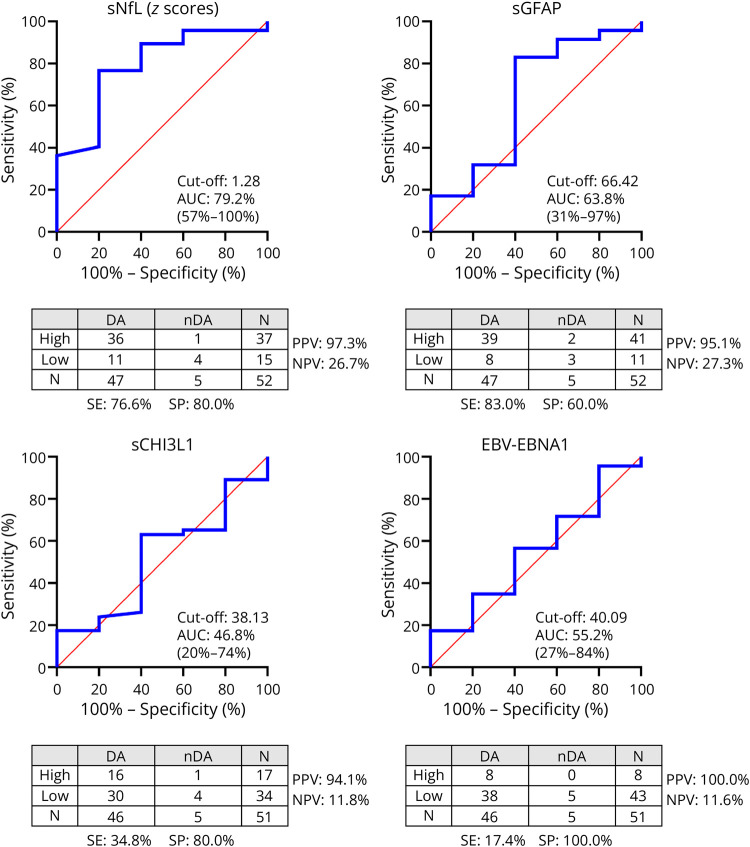
Results: We included 181 patients (66.3% females, mean [SD] age of 35.0 [9.7] years). At baseline, 25 (13.8%) were classified as noDIS and noDIT, 62 (34.3%) as DIS and noDIT, and 94 (51.9%) as DIS and DIT. Only sNfL Z-scores discriminated between groups (DIS and DIT vs DIS and noDIT [p = 0.002], DIS and DIT vs noDIS and noDIT [p < 0.001], and DIS and noDIT vs noDIS and noDIT [p = 0.026]). In noDIS and noDIT patients (median interquartile range [IQR] follow-up of 8.1 [5.0-11.7] years), high sNfL Z-scores best predicted MS diagnosis (specificity [SP] and 95% CI of 93.3% [68.1-99.8] and positive predictive value [PPV] of 87.5% [47.3-99.7]). Among DIS and noDIT patients (median [IQR] follow-up of 6.8 [4.0-9.1] years), high sNfL Z-scores best predicted MS diagnosis (SP of 80% [28.4-99.5] and PPV of 97.3% [85.8-99.9]) without considering oligoclonal band (OB) status. In the subset of patients of this group with negative OBs, a combination of high sNfL Z-scores and sGFAP levels predicted MS diagnosis (SP of 100% [39.8-100] and PPV of 100% [54.1-100]).
Discussion: These results suggest that sNfL and sGFAP may be incorporated in particular scenarios to diagnose MS in patients with CIS not fulfilling current diagnostic criteria.
期刊介绍:
Neurology Neuroimmunology & Neuroinflammation is an official journal of the American Academy of Neurology. Neurology: Neuroimmunology & Neuroinflammation will be the premier peer-reviewed journal in neuroimmunology and neuroinflammation. This journal publishes rigorously peer-reviewed open-access reports of original research and in-depth reviews of topics in neuroimmunology & neuroinflammation, affecting the full range of neurologic diseases including (but not limited to) Alzheimer's disease, Parkinson's disease, ALS, tauopathy, and stroke; multiple sclerosis and NMO; inflammatory peripheral nerve and muscle disease, Guillain-Barré and myasthenia gravis; nervous system infection; paraneoplastic syndromes, noninfectious encephalitides and other antibody-mediated disorders; and psychiatric and neurodevelopmental disorders. Clinical trials, instructive case reports, and small case series will also be featured.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


