Yogita S Patel, Forough Farrokhyar, Marko Simunovic, Waël C Hanna
{"title":"近红外荧光引导的节段切除术:吲哚菁绿染料的额外益处随着外科医生经验的减少而减少。","authors":"Yogita S Patel, Forough Farrokhyar, Marko Simunovic, Waël C Hanna","doi":"10.1177/15533506251315979","DOIUrl":null,"url":null,"abstract":"<p><p>BackgroundNear-infrared fluorescence (NIF)-mapping with indocyanine green dye (ICG) facilitates the identification of the intersegmental plane during minimally invasive segmentectomy. Our pilot study showed that ICG is associated with an increase in oncological margin distance from the tumour, greater than the surgeon's best judgment. We hypothesized that, with greater experience, the surgeon's judgement will improve, and the benefit of ICG will diminish.MethodsThis is a phase 2 single-arm trial of patients undergoing robotic-assisted segmentectomy for NSCLC tumours less than 3 cm. After isolating the diseased segment(s), the predicted intersegmental plane (Dp) was identified by the thoracic surgeon. After intravenous ICG injection, the true intersegmental plane (Dt) was revealed using NIF. The primary outcome was the average distance between Dt and Dp (Dt-Dp). Comparisons were performed across 3 temporal tertiles: tertile 1 (t1) comprised of the first 30 participants, and the remaining participants were divided equally for tertiles 2 (t2) and 3 (t3). Kruskal-Wallis test was used to compare differences between tertiles (α = 0.05).ResultsA total of 190 patients were enrolled from October 2016 to June 2021. The median age was 68 (interquartile range:62-72), and 57.37%(109/190) were women. ICG injection occurred in 60.53%(115/190) of the participants, and intersegmental plane visualization was achieved in 88.70%(102/115). Dt-Dp diminished significantly across tertiles: t1 = 20.65 ± 15.82 mm, t2 = 2.42 ± 15.49 mm, and t3 = 1.36 ± 9.87 mm (<i>P</i> = 0.0001). Locally estimated scatterplot smoothing revealed that this distance approaches zero as the surgeon performs more cases.ConclusionIn our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added value of NIF-mapping with ICG diminishes with surgeon experience.</p>","PeriodicalId":22095,"journal":{"name":"Surgical Innovation","volume":" ","pages":"211-221"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12022369/pdf/","citationCount":"0","resultStr":"{\"title\":\"Near-Infrared Fluorescence-Guided Segmentectomy: Added Benefit of Indocyanine Green Dye Diminishes With Surgeon Experience.\",\"authors\":\"Yogita S Patel, Forough Farrokhyar, Marko Simunovic, Waël C Hanna\",\"doi\":\"10.1177/15533506251315979\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BackgroundNear-infrared fluorescence (NIF)-mapping with indocyanine green dye (ICG) facilitates the identification of the intersegmental plane during minimally invasive segmentectomy. Our pilot study showed that ICG is associated with an increase in oncological margin distance from the tumour, greater than the surgeon's best judgment. We hypothesized that, with greater experience, the surgeon's judgement will improve, and the benefit of ICG will diminish.MethodsThis is a phase 2 single-arm trial of patients undergoing robotic-assisted segmentectomy for NSCLC tumours less than 3 cm. After isolating the diseased segment(s), the predicted intersegmental plane (Dp) was identified by the thoracic surgeon. After intravenous ICG injection, the true intersegmental plane (Dt) was revealed using NIF. The primary outcome was the average distance between Dt and Dp (Dt-Dp). Comparisons were performed across 3 temporal tertiles: tertile 1 (t1) comprised of the first 30 participants, and the remaining participants were divided equally for tertiles 2 (t2) and 3 (t3). Kruskal-Wallis test was used to compare differences between tertiles (α = 0.05).ResultsA total of 190 patients were enrolled from October 2016 to June 2021. The median age was 68 (interquartile range:62-72), and 57.37%(109/190) were women. ICG injection occurred in 60.53%(115/190) of the participants, and intersegmental plane visualization was achieved in 88.70%(102/115). Dt-Dp diminished significantly across tertiles: t1 = 20.65 ± 15.82 mm, t2 = 2.42 ± 15.49 mm, and t3 = 1.36 ± 9.87 mm (<i>P</i> = 0.0001). Locally estimated scatterplot smoothing revealed that this distance approaches zero as the surgeon performs more cases.ConclusionIn our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added value of NIF-mapping with ICG diminishes with surgeon experience.</p>\",\"PeriodicalId\":22095,\"journal\":{\"name\":\"Surgical Innovation\",\"volume\":\" \",\"pages\":\"211-221\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12022369/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Innovation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/15533506251315979\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Innovation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/15533506251315979","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/22 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
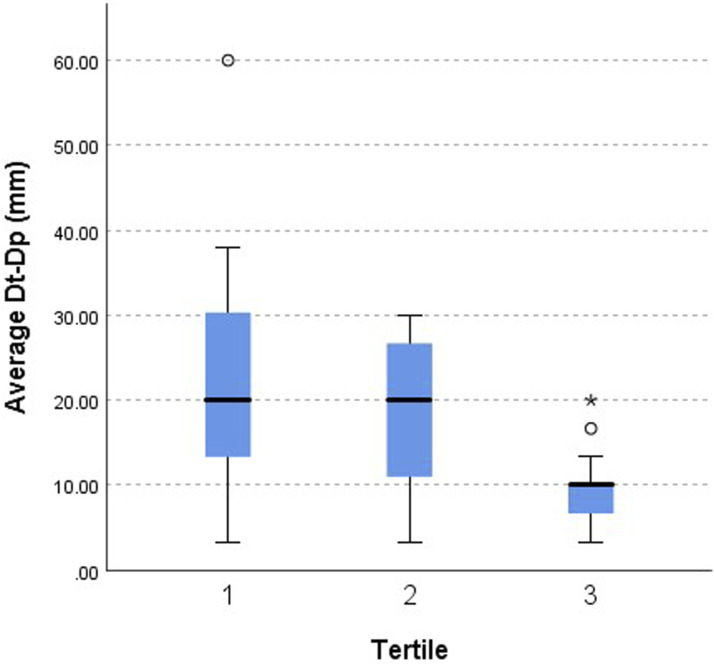
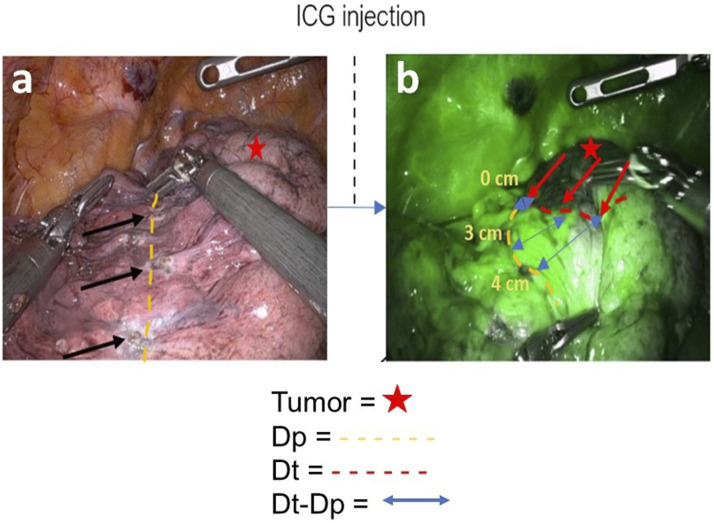
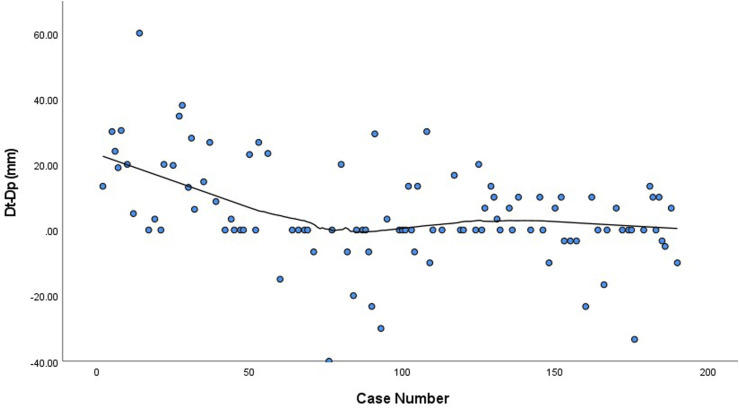
背景:近红外荧光(NIF)与吲哚菁绿染料(ICG)的定位有助于在微创节段切除术中识别节段间平面。我们的初步研究表明,ICG与肿瘤边缘距离的增加有关,大于外科医生的最佳判断。我们假设,随着经验的增加,外科医生的判断将会提高,ICG的好处将会减少。方法:这是一项2期单臂试验,患者接受机器人辅助的非小细胞肺癌(NSCLC)节段切除术,治疗小于3cm的肿瘤。分离病变节段后,胸外科医生确定预测的节段间平面(Dp)。静脉注射ICG后,用NIF显示真实节段间平面(Dt)。主要终点是Dt和Dp之间的平均距离(Dt-Dp)。在三个时间分位数中进行比较:分位数1 (t1)由前30名参与者组成,其余参与者平均分为分位数2 (t2)和3 (t3)。采用Kruskal-Wallis检验比较各组间差异(α = 0.05)。结果:2016年10月至2021年6月共入组190例患者。中位年龄为68岁(四分位数范围:62-72),57.37%(109/190)为女性。60.53%(115/190)的参与者注射了ICG, 88.70%(102/115)的参与者实现了节段间平面显示。t1 = 20.65±15.82 mm, t2 = 2.42±15.49 mm, t3 = 1.36±9.87 mm (P = 0.0001)。局部估计的散点图平滑显示,随着手术次数的增加,这个距离接近于零。结论:在我们的单外科医生机器人辅助非小细胞肺癌节段切除术的经验中,ICG的nif制图的附加价值随着外科医生经验的增加而减少。
Near-Infrared Fluorescence-Guided Segmentectomy: Added Benefit of Indocyanine Green Dye Diminishes With Surgeon Experience.
BackgroundNear-infrared fluorescence (NIF)-mapping with indocyanine green dye (ICG) facilitates the identification of the intersegmental plane during minimally invasive segmentectomy. Our pilot study showed that ICG is associated with an increase in oncological margin distance from the tumour, greater than the surgeon's best judgment. We hypothesized that, with greater experience, the surgeon's judgement will improve, and the benefit of ICG will diminish.MethodsThis is a phase 2 single-arm trial of patients undergoing robotic-assisted segmentectomy for NSCLC tumours less than 3 cm. After isolating the diseased segment(s), the predicted intersegmental plane (Dp) was identified by the thoracic surgeon. After intravenous ICG injection, the true intersegmental plane (Dt) was revealed using NIF. The primary outcome was the average distance between Dt and Dp (Dt-Dp). Comparisons were performed across 3 temporal tertiles: tertile 1 (t1) comprised of the first 30 participants, and the remaining participants were divided equally for tertiles 2 (t2) and 3 (t3). Kruskal-Wallis test was used to compare differences between tertiles (α = 0.05).ResultsA total of 190 patients were enrolled from October 2016 to June 2021. The median age was 68 (interquartile range:62-72), and 57.37%(109/190) were women. ICG injection occurred in 60.53%(115/190) of the participants, and intersegmental plane visualization was achieved in 88.70%(102/115). Dt-Dp diminished significantly across tertiles: t1 = 20.65 ± 15.82 mm, t2 = 2.42 ± 15.49 mm, and t3 = 1.36 ± 9.87 mm (P = 0.0001). Locally estimated scatterplot smoothing revealed that this distance approaches zero as the surgeon performs more cases.ConclusionIn our single-surgeon experience with robotic-assisted segmentectomy for NSCLC, the added value of NIF-mapping with ICG diminishes with surgeon experience.
期刊介绍:
Surgical Innovation (SRI) is a peer-reviewed bi-monthly journal focusing on minimally invasive surgical techniques, new instruments such as laparoscopes and endoscopes, and new technologies. SRI prepares surgeons to think and work in "the operating room of the future" through learning new techniques, understanding and adapting to new technologies, maintaining surgical competencies, and applying surgical outcomes data to their practices. This journal is a member of the Committee on Publication Ethics (COPE).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


