Prediction of pre-eclampsia using maternal hemodynamic parameters at 12 + 0 to 15 + 6 weeks.
Objectives: To compare the maternal hemodynamic profile at 12 + 0 to 15 + 6 weeks' gestation in women who subsequently developed pre-eclampsia (PE) and those who did not, and to assess the screening performance of maternal hemodynamic parameters for PE in combination with the Fetal Medicine Foundation (FMF) triple test, including maternal factors (MF), mean arterial pressure (MAP), uterine artery pulsatility index and placental growth factor.
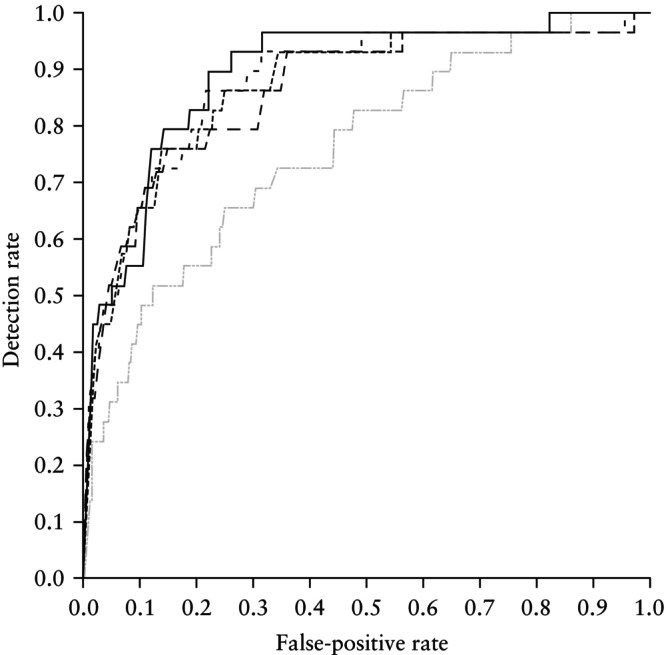
Methods: This was a prospective case-control study involving Chinese women with a singleton pregnancy who underwent preterm PE screening at 11 + 0 to 13 + 6 weeks' gestation using the FMF triple test, between February 2020 and February 2023. Women identified as being at high risk (≥ 1:100) for preterm PE by the FMF triple test were matched 1:1 with women identified as low risk (< 1:100) for maternal age ± 3 years, maternal weight ± 5 kg and date of screening ± 14 days. Two-dimensional transthoracic echocardiography was performed at 12 + 0 to 15 + 6 weeks to evaluate maternal hemodynamic parameters (heart rate (HR), stroke volume (SV), cardiac output (CO) and systemic vascular resistance (SVR)). Maternal hemodynamic parameters were expressed as multiples of the median (MoM) values, determined by linear regression models to adjust for gestational age (GA) and MF. The distribution of log10 MoM values of maternal hemodynamic parameters in cases of PE and unaffected pregnancies, and the association between these hemodynamic parameters and GA at delivery, were assessed. The risks of preterm PE (delivery before 37 weeks) and any-onset PE (delivery at any time) were reassessed using Bayes' theorem after maternal hemodynamic parameters were added to the FMF triple test. The screening performance for preterm PE and any-onset PE was determined by the area under the receiver-operating-characteristics curve (AUC) and detection rate at a 10% fixed false-positive rate (FPR). Differences in AUC (ΔAUC) were assessed using DeLong's test.
Results: A total of 743 cases were analyzed, of whom 39 (5.2%) subsequently developed PE, including 29 (3.9%) cases of preterm PE and 10 (1.3%) cases of term PE. Mean log10 SVR MoM was significantly higher in cases of preterm PE and any-onset PE compared with unaffected pregnancies. Mean log10 SV MoM and log10 CO MoM were significantly lower in cases of preterm PE and any-onset PE compared with unaffected pregnancies. Mean log10 HR MoM was not significantly different between the study groups. Mean log10 CO MoM and log10 SVR MoM were not significantly correlated with GA at delivery in preterm PE and any-onset PE. For the prediction of preterm PE and any-onset PE, adding CO or SVR or replacing MAP with CO and SVR in the FMF triple test achieved an identical or greater AUC compared with the FMF triple test, but ΔAUC was not significantly different. In addition, adding CO or SVR or replacing MAP by CO and SVR in the FMF triple test did not improve the detection rate for preterm PE and any-onset PE at a fixed FPR of 10%.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


