Elisabeth Day, Deborah Cross, David Crossland, Jason Powell, Emma Simpson
{"title":"气管切开术作为儿科心脏移植后的治疗选择。","authors":"Elisabeth Day, Deborah Cross, David Crossland, Jason Powell, Emma Simpson","doi":"10.1111/petr.70029","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Children with end-stage heart failure listed for cardiac transplantation may require mechanical ventilation and/or circulatory support whilst awaiting transplantation. A subgroup of these patients is unable to wean off mechanical ventilator support and undergo tracheostomy to enhance quality of life and allow de-escalation of intensive care. There is limited evidence of the use of tracheostomy associated with pediatric cardiac transplantation. We describe outcomes to better inform future management of these patients.</p><p><strong>Methods: </strong>A single-centre, retrospective study was performed, assessing all pediatric patients (< 18 years) listed for cardiac transplant from 2006 to 2017. We assessed background demographics and outcomes, including cardiac diagnosis, complications, insertion of ventricular assist device and survival. We identified patients who underwent tracheostomy after listing and compared this group with non-tracheostomised patients.</p><p><strong>Results: </strong>Two hundred and eleven patients were listed for cardiac transplant, of whom 44 (21%) underwent tracheostomy after listing. The main indication for tracheostomy was failure to wean from mechanical ventilation (36%). Complications after tracheostomy included localized infection, granuloma, obstruction and hemorrhage, but were generally minor. Median time for tracheostomy decannulation was 75 days. When comparing tracheostomy versus non-tracheostomy patients, there were no significant differences in age, weight or time to transplant. Survival was comparable between the non-tracheostomy and tracheostomy groups at 1-year, 97% versus 94% respectively.</p><p><strong>Conclusion: </strong>There is no evidence from our study that patients awaiting cardiac transplant who undergo tracheostomy have significant complications or reduced survival. Tracheostomy is usually a short-term measure and should be considered in the management of children receiving prolonged ventilation around the time of cardiac transplantation.</p>","PeriodicalId":20038,"journal":{"name":"Pediatric Transplantation","volume":"29 1","pages":"e70029"},"PeriodicalIF":1.4000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11750632/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tracheostomy as a Management Option After Listing for Pediatric Cardiac Transplantation.\",\"authors\":\"Elisabeth Day, Deborah Cross, David Crossland, Jason Powell, Emma Simpson\",\"doi\":\"10.1111/petr.70029\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Children with end-stage heart failure listed for cardiac transplantation may require mechanical ventilation and/or circulatory support whilst awaiting transplantation. A subgroup of these patients is unable to wean off mechanical ventilator support and undergo tracheostomy to enhance quality of life and allow de-escalation of intensive care. There is limited evidence of the use of tracheostomy associated with pediatric cardiac transplantation. We describe outcomes to better inform future management of these patients.</p><p><strong>Methods: </strong>A single-centre, retrospective study was performed, assessing all pediatric patients (< 18 years) listed for cardiac transplant from 2006 to 2017. We assessed background demographics and outcomes, including cardiac diagnosis, complications, insertion of ventricular assist device and survival. We identified patients who underwent tracheostomy after listing and compared this group with non-tracheostomised patients.</p><p><strong>Results: </strong>Two hundred and eleven patients were listed for cardiac transplant, of whom 44 (21%) underwent tracheostomy after listing. The main indication for tracheostomy was failure to wean from mechanical ventilation (36%). Complications after tracheostomy included localized infection, granuloma, obstruction and hemorrhage, but were generally minor. Median time for tracheostomy decannulation was 75 days. When comparing tracheostomy versus non-tracheostomy patients, there were no significant differences in age, weight or time to transplant. Survival was comparable between the non-tracheostomy and tracheostomy groups at 1-year, 97% versus 94% respectively.</p><p><strong>Conclusion: </strong>There is no evidence from our study that patients awaiting cardiac transplant who undergo tracheostomy have significant complications or reduced survival. Tracheostomy is usually a short-term measure and should be considered in the management of children receiving prolonged ventilation around the time of cardiac transplantation.</p>\",\"PeriodicalId\":20038,\"journal\":{\"name\":\"Pediatric Transplantation\",\"volume\":\"29 1\",\"pages\":\"e70029\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11750632/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Transplantation\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/petr.70029\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Transplantation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/petr.70029","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Tracheostomy as a Management Option After Listing for Pediatric Cardiac Transplantation.
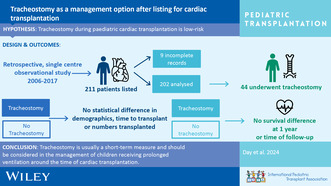
Background: Children with end-stage heart failure listed for cardiac transplantation may require mechanical ventilation and/or circulatory support whilst awaiting transplantation. A subgroup of these patients is unable to wean off mechanical ventilator support and undergo tracheostomy to enhance quality of life and allow de-escalation of intensive care. There is limited evidence of the use of tracheostomy associated with pediatric cardiac transplantation. We describe outcomes to better inform future management of these patients.
Methods: A single-centre, retrospective study was performed, assessing all pediatric patients (< 18 years) listed for cardiac transplant from 2006 to 2017. We assessed background demographics and outcomes, including cardiac diagnosis, complications, insertion of ventricular assist device and survival. We identified patients who underwent tracheostomy after listing and compared this group with non-tracheostomised patients.
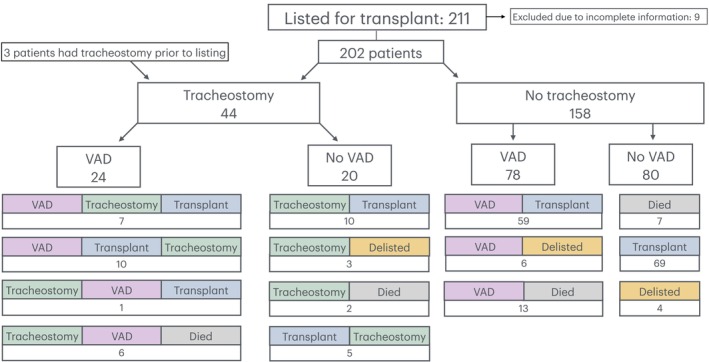
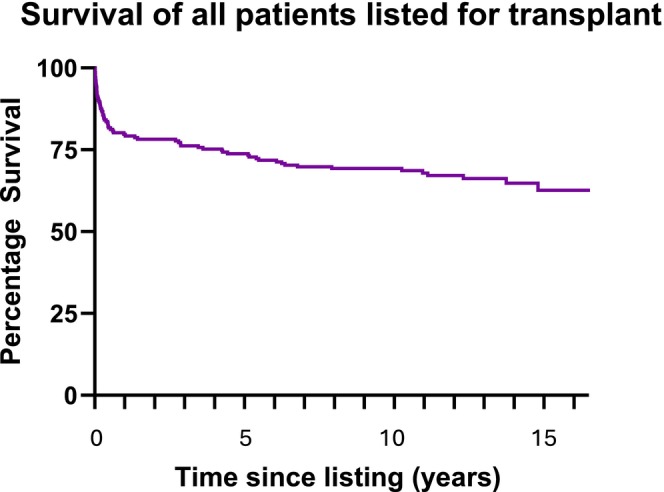
Results: Two hundred and eleven patients were listed for cardiac transplant, of whom 44 (21%) underwent tracheostomy after listing. The main indication for tracheostomy was failure to wean from mechanical ventilation (36%). Complications after tracheostomy included localized infection, granuloma, obstruction and hemorrhage, but were generally minor. Median time for tracheostomy decannulation was 75 days. When comparing tracheostomy versus non-tracheostomy patients, there were no significant differences in age, weight or time to transplant. Survival was comparable between the non-tracheostomy and tracheostomy groups at 1-year, 97% versus 94% respectively.
Conclusion: There is no evidence from our study that patients awaiting cardiac transplant who undergo tracheostomy have significant complications or reduced survival. Tracheostomy is usually a short-term measure and should be considered in the management of children receiving prolonged ventilation around the time of cardiac transplantation.
期刊介绍:
The aim of Pediatric Transplantation is to publish original articles of the highest quality on clinical experience and basic research in transplantation of tissues and solid organs in infants, children and adolescents. The journal seeks to disseminate the latest information widely to all individuals involved in kidney, liver, heart, lung, intestine and stem cell (bone-marrow) transplantation. In addition, the journal publishes focused reviews on topics relevant to pediatric transplantation as well as timely editorial comment on controversial issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


