Zachary M Stauber, Quinn T Ehlen, Nicholas A Mirsky, Marshall E Stauber
{"title":"纹状棒状杆菌败血症合并术后骨髓炎需要补救性椎体切除的后凸成形术:1例报告。","authors":"Zachary M Stauber, Quinn T Ehlen, Nicholas A Mirsky, Marshall E Stauber","doi":"10.21037/jss-24-31","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Kyphoplasty (KP) is a well-established procedure with a low complication risk, however, the procedure's safety in patients with comorbidities and in the setting of systemic infection remains uncertain with no clear guidelines. We present a unique case of KP in the setting of recurrent septicemia, which required subsequent salvage vertebrectomy.</p><p><strong>Case description: </strong>We present a clinical case of a 59-year-old diabetic male patient with a recent foot ulcer, positive for <i>Corynebacterium striatum</i> and <i>Enterococcus</i>. Shortly after discharge, the patient was admitted for signs of septicemia positive for <i>Corynebacterium striatum</i> and <i>Pseudomonas aeruginosa</i>. The patient had also sustained an acute L1 compression fracture at the time of septic presentation. A KP was performed, just 10 days after original septicemia diagnosis. 5 months later, the patient presented with continued incapacitating back pain at the operative site, and a diagnose revealing osteomyelitis at the location of the L1 KP positive for <i>Corynebacterium striatum</i>, treated with vancomycin and daptomycin. The cement and surrounding bone were compromised and instability developed, requiring an L1 vertebrectomy with T9-L4 posterior fusion with allograft. The patient has been followed for 1.5 years postoperatively with full recovery, decreased pain, and improved quality of life. We discuss the importance of KP safety in the setting of recurrent systemic infection.</p><p><strong>Conclusions: </strong>While current cases in literature discuss the infectious risk of KP, this case emphasizes the extended time in which osteomyelitis can recur in patient with systemic infections. Care must be taken preoperatively and perioperatively to ensure there is minimal risk of further bacterial seeding into implanted materials. Preoperative infection status should be monitored via blood culture and inflammatory markers. Preoperative and perioperative antibiotics should be administered and perioperative cultures should be collected in case of postoperative infection. Further cases, prospective, and retrospective studies are necessary to fully understand the adequate guidelines to performing KP in the setting of systemic infection.</p>","PeriodicalId":17131,"journal":{"name":"Journal of spine surgery","volume":"10 4","pages":"724-732"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732315/pdf/","citationCount":"0","resultStr":"{\"title\":\"Kyphoplasty in the setting of corynebacterium striatum septicemia with postoperative osteomyelitis requiring salvage vertebrectomy: a case report.\",\"authors\":\"Zachary M Stauber, Quinn T Ehlen, Nicholas A Mirsky, Marshall E Stauber\",\"doi\":\"10.21037/jss-24-31\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Kyphoplasty (KP) is a well-established procedure with a low complication risk, however, the procedure's safety in patients with comorbidities and in the setting of systemic infection remains uncertain with no clear guidelines. We present a unique case of KP in the setting of recurrent septicemia, which required subsequent salvage vertebrectomy.</p><p><strong>Case description: </strong>We present a clinical case of a 59-year-old diabetic male patient with a recent foot ulcer, positive for <i>Corynebacterium striatum</i> and <i>Enterococcus</i>. Shortly after discharge, the patient was admitted for signs of septicemia positive for <i>Corynebacterium striatum</i> and <i>Pseudomonas aeruginosa</i>. The patient had also sustained an acute L1 compression fracture at the time of septic presentation. A KP was performed, just 10 days after original septicemia diagnosis. 5 months later, the patient presented with continued incapacitating back pain at the operative site, and a diagnose revealing osteomyelitis at the location of the L1 KP positive for <i>Corynebacterium striatum</i>, treated with vancomycin and daptomycin. The cement and surrounding bone were compromised and instability developed, requiring an L1 vertebrectomy with T9-L4 posterior fusion with allograft. The patient has been followed for 1.5 years postoperatively with full recovery, decreased pain, and improved quality of life. We discuss the importance of KP safety in the setting of recurrent systemic infection.</p><p><strong>Conclusions: </strong>While current cases in literature discuss the infectious risk of KP, this case emphasizes the extended time in which osteomyelitis can recur in patient with systemic infections. Care must be taken preoperatively and perioperatively to ensure there is minimal risk of further bacterial seeding into implanted materials. Preoperative infection status should be monitored via blood culture and inflammatory markers. Preoperative and perioperative antibiotics should be administered and perioperative cultures should be collected in case of postoperative infection. Further cases, prospective, and retrospective studies are necessary to fully understand the adequate guidelines to performing KP in the setting of systemic infection.</p>\",\"PeriodicalId\":17131,\"journal\":{\"name\":\"Journal of spine surgery\",\"volume\":\"10 4\",\"pages\":\"724-732\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11732315/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of spine surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.21037/jss-24-31\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of spine surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/jss-24-31","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/5 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Kyphoplasty in the setting of corynebacterium striatum septicemia with postoperative osteomyelitis requiring salvage vertebrectomy: a case report.
Background: Kyphoplasty (KP) is a well-established procedure with a low complication risk, however, the procedure's safety in patients with comorbidities and in the setting of systemic infection remains uncertain with no clear guidelines. We present a unique case of KP in the setting of recurrent septicemia, which required subsequent salvage vertebrectomy.
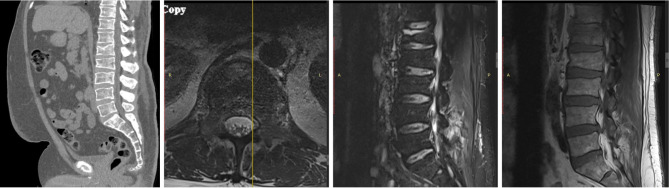
Case description: We present a clinical case of a 59-year-old diabetic male patient with a recent foot ulcer, positive for Corynebacterium striatum and Enterococcus. Shortly after discharge, the patient was admitted for signs of septicemia positive for Corynebacterium striatum and Pseudomonas aeruginosa. The patient had also sustained an acute L1 compression fracture at the time of septic presentation. A KP was performed, just 10 days after original septicemia diagnosis. 5 months later, the patient presented with continued incapacitating back pain at the operative site, and a diagnose revealing osteomyelitis at the location of the L1 KP positive for Corynebacterium striatum, treated with vancomycin and daptomycin. The cement and surrounding bone were compromised and instability developed, requiring an L1 vertebrectomy with T9-L4 posterior fusion with allograft. The patient has been followed for 1.5 years postoperatively with full recovery, decreased pain, and improved quality of life. We discuss the importance of KP safety in the setting of recurrent systemic infection.
Conclusions: While current cases in literature discuss the infectious risk of KP, this case emphasizes the extended time in which osteomyelitis can recur in patient with systemic infections. Care must be taken preoperatively and perioperatively to ensure there is minimal risk of further bacterial seeding into implanted materials. Preoperative infection status should be monitored via blood culture and inflammatory markers. Preoperative and perioperative antibiotics should be administered and perioperative cultures should be collected in case of postoperative infection. Further cases, prospective, and retrospective studies are necessary to fully understand the adequate guidelines to performing KP in the setting of systemic infection.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


