{"title":"免疫异常和22q11.2缺失在conotruncal异常儿童中的患病率:一项横断面研究。","authors":"Souvik Das, Arun Kumar Baranwal, Amit Rawat, Ashwini Nair, Sanjeev Hanumantacharya Naganur, Anupriya Kaur, Anand Kumar Mishra, Ankur Jindal, Anit Kaur","doi":"10.4103/apc.apc_168_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>22q11.2 deletion is associated with conotruncal anomalies and immunological aberrations. Given the common embryonic origin of conotruncus and thymus, conotruncal anomalies may be associated with immunological aberrations irrespective of 22q11.2 deletion. We planned to study the prevalence of immunological aberrations and 22q11.2 deletion among patients with conotruncal anomaly to understand the impact of their interplay.</p><p><strong>Patients and methods: </strong>Preoperative children (age <12 years) with conotruncal anomalies were evaluated for clinical dysmorphism, lymphocyte subsets by flowcytometry, immunoglobulin levels by nephelometry, and 22q11.2 deletion by multiplex ligand-dependent probe amplification (January 2021-June 2022). Patients with asplenia and polysplenia were excluded from immunological studies.</p><p><strong>Results: </strong>Major cardiac defects ([<i>n</i> = 101], [median age, 32 days]) included dextro-transposition of great arteries (d-TGA) - 41.6%, tetralogy of Fallot - 37.6%, double outlet right ventricle (DORV) - 13.9%, and truncus arteriosus - 4.9%. Four patients had polysplenia with situs inversus, while 17 had clinical dysmorphism. Flow cytometry (<i>n</i> = 82) revealed low absolute counts of lymphocytes (33%), T-cells (51.2%), CD4+ cells (50%), and CD8+ cells (51.2%), while only 14.1% had low IgG levels. Eight patients (8/95, 8.4%) had 22q11.2 deletion, with universal deletion of <i>TBX1-2</i> and <i>TBX1-7 genes</i>; the other 19 genes were deleted in various combinations. Two patients with 22q11.2 deletion had normal T-cell subsets, while none had a complete absence of T-cells.</p><p><strong>Conclusion: </strong>Immunological aberrations, especially T-cell abnormalities, were present in almost half of the patients, irrespective of 22q11.2 deletion. Only 8.4% of patients had 22q11.2 deletion. The high incidence of d-TGA among 22q11.2 deletion patients needs further exploration.</p>","PeriodicalId":8026,"journal":{"name":"Annals of Pediatric Cardiology","volume":"17 5","pages":"339-346"},"PeriodicalIF":0.7000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737628/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevalence of immunological aberrations and 22q11.2 deletion in children with conotruncal anomalies: A cross-sectional study.\",\"authors\":\"Souvik Das, Arun Kumar Baranwal, Amit Rawat, Ashwini Nair, Sanjeev Hanumantacharya Naganur, Anupriya Kaur, Anand Kumar Mishra, Ankur Jindal, Anit Kaur\",\"doi\":\"10.4103/apc.apc_168_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>22q11.2 deletion is associated with conotruncal anomalies and immunological aberrations. Given the common embryonic origin of conotruncus and thymus, conotruncal anomalies may be associated with immunological aberrations irrespective of 22q11.2 deletion. We planned to study the prevalence of immunological aberrations and 22q11.2 deletion among patients with conotruncal anomaly to understand the impact of their interplay.</p><p><strong>Patients and methods: </strong>Preoperative children (age <12 years) with conotruncal anomalies were evaluated for clinical dysmorphism, lymphocyte subsets by flowcytometry, immunoglobulin levels by nephelometry, and 22q11.2 deletion by multiplex ligand-dependent probe amplification (January 2021-June 2022). Patients with asplenia and polysplenia were excluded from immunological studies.</p><p><strong>Results: </strong>Major cardiac defects ([<i>n</i> = 101], [median age, 32 days]) included dextro-transposition of great arteries (d-TGA) - 41.6%, tetralogy of Fallot - 37.6%, double outlet right ventricle (DORV) - 13.9%, and truncus arteriosus - 4.9%. Four patients had polysplenia with situs inversus, while 17 had clinical dysmorphism. Flow cytometry (<i>n</i> = 82) revealed low absolute counts of lymphocytes (33%), T-cells (51.2%), CD4+ cells (50%), and CD8+ cells (51.2%), while only 14.1% had low IgG levels. Eight patients (8/95, 8.4%) had 22q11.2 deletion, with universal deletion of <i>TBX1-2</i> and <i>TBX1-7 genes</i>; the other 19 genes were deleted in various combinations. Two patients with 22q11.2 deletion had normal T-cell subsets, while none had a complete absence of T-cells.</p><p><strong>Conclusion: </strong>Immunological aberrations, especially T-cell abnormalities, were present in almost half of the patients, irrespective of 22q11.2 deletion. Only 8.4% of patients had 22q11.2 deletion. The high incidence of d-TGA among 22q11.2 deletion patients needs further exploration.</p>\",\"PeriodicalId\":8026,\"journal\":{\"name\":\"Annals of Pediatric Cardiology\",\"volume\":\"17 5\",\"pages\":\"339-346\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737628/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Pediatric Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/apc.apc_168_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/apc.apc_168_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Prevalence of immunological aberrations and 22q11.2 deletion in children with conotruncal anomalies: A cross-sectional study.
Introduction: 22q11.2 deletion is associated with conotruncal anomalies and immunological aberrations. Given the common embryonic origin of conotruncus and thymus, conotruncal anomalies may be associated with immunological aberrations irrespective of 22q11.2 deletion. We planned to study the prevalence of immunological aberrations and 22q11.2 deletion among patients with conotruncal anomaly to understand the impact of their interplay.
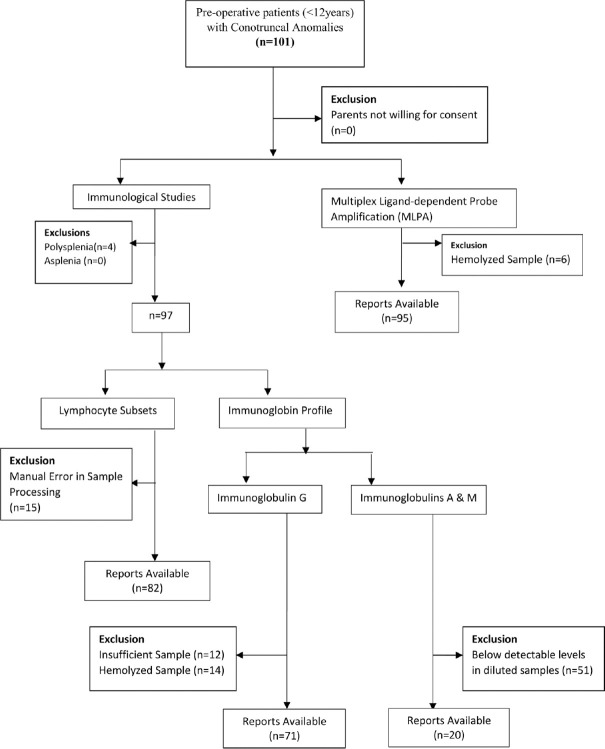
Patients and methods: Preoperative children (age <12 years) with conotruncal anomalies were evaluated for clinical dysmorphism, lymphocyte subsets by flowcytometry, immunoglobulin levels by nephelometry, and 22q11.2 deletion by multiplex ligand-dependent probe amplification (January 2021-June 2022). Patients with asplenia and polysplenia were excluded from immunological studies.
Results: Major cardiac defects ([n = 101], [median age, 32 days]) included dextro-transposition of great arteries (d-TGA) - 41.6%, tetralogy of Fallot - 37.6%, double outlet right ventricle (DORV) - 13.9%, and truncus arteriosus - 4.9%. Four patients had polysplenia with situs inversus, while 17 had clinical dysmorphism. Flow cytometry (n = 82) revealed low absolute counts of lymphocytes (33%), T-cells (51.2%), CD4+ cells (50%), and CD8+ cells (51.2%), while only 14.1% had low IgG levels. Eight patients (8/95, 8.4%) had 22q11.2 deletion, with universal deletion of TBX1-2 and TBX1-7 genes; the other 19 genes were deleted in various combinations. Two patients with 22q11.2 deletion had normal T-cell subsets, while none had a complete absence of T-cells.
Conclusion: Immunological aberrations, especially T-cell abnormalities, were present in almost half of the patients, irrespective of 22q11.2 deletion. Only 8.4% of patients had 22q11.2 deletion. The high incidence of d-TGA among 22q11.2 deletion patients needs further exploration.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


