Nikita Panigrahi, Harohalli A Venkatesh, Manas Ranjan Mishra, Rajath Pejaver, Karthik N Nagesh
{"title":"比较新生儿呼吸窘迫恢复前后的组织多普勒左心室心肌功能指数:一项前瞻性观察研究。","authors":"Nikita Panigrahi, Harohalli A Venkatesh, Manas Ranjan Mishra, Rajath Pejaver, Karthik N Nagesh","doi":"10.4103/apc.apc_167_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Respiratory distress is the most common cause requiring neonatal intensive care unit admission. As respiratory and cardiac functions are closely interrelated, some cardiac dysfunction is expected in respiratory distress. The myocardial performance index (MPI) is an index to assess global myocardial function, easily measurable by bedside echocardiography and reliable. Here, we conducted this study to determine the change in cardiac function in neonates with respiratory distress before initiating respiratory support and after weaning from the support.</p><p><strong>Methodology: </strong>The study was carried out in 92 neonates with a gestational age of more than 32 weeks who required invasive or noninvasive respiratory support. The tissue Doppler left ventricular MPI (LV MPI) was calculated before the initiation of respiratory support and after weaning from respiratory support. The data were analyzed using a paired <i>t</i>-test and a Wilcoxon signed-rank test.</p><p><strong>Results: </strong>This study comprised 92 neonates with a median (interquartile range) LV MPI value of 0.56 (0.10) before initiation of respiratory support and 0.47 (0.04) after weaning from respiratory support with <i>P</i> < 0.001. The isovolumetric contraction time, isovolumetric relaxation time, and ejection time increased after weaning from respiratory support (all <i>P</i> < 0.0001). The severity of respiratory distress determined by invasive mode of ventilation and longer duration of respiratory support caused higher initial LV MPI before initiation of respiratory support compared with recovery and <i>P</i> < 0.001, suggesting subclinical ventricular dysfunction with respiratory distress in neonates.</p><p><strong>Conclusion: </strong>LV MPI was higher in neonates with respiratory distress and normalized after weaning from respiratory support, which indicates that neonates requiring respiratory support may have subclinical ventricular dysfunction and should be followed up carefully.</p>","PeriodicalId":8026,"journal":{"name":"Annals of Pediatric Cardiology","volume":"17 5","pages":"331-338"},"PeriodicalIF":0.7000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737619/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparing the tissue Doppler-derived left ventricular myocardial performance index before and after recovery from respiratory distress in neonates: A prospective observational study.\",\"authors\":\"Nikita Panigrahi, Harohalli A Venkatesh, Manas Ranjan Mishra, Rajath Pejaver, Karthik N Nagesh\",\"doi\":\"10.4103/apc.apc_167_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objective: </strong>Respiratory distress is the most common cause requiring neonatal intensive care unit admission. As respiratory and cardiac functions are closely interrelated, some cardiac dysfunction is expected in respiratory distress. The myocardial performance index (MPI) is an index to assess global myocardial function, easily measurable by bedside echocardiography and reliable. Here, we conducted this study to determine the change in cardiac function in neonates with respiratory distress before initiating respiratory support and after weaning from the support.</p><p><strong>Methodology: </strong>The study was carried out in 92 neonates with a gestational age of more than 32 weeks who required invasive or noninvasive respiratory support. The tissue Doppler left ventricular MPI (LV MPI) was calculated before the initiation of respiratory support and after weaning from respiratory support. The data were analyzed using a paired <i>t</i>-test and a Wilcoxon signed-rank test.</p><p><strong>Results: </strong>This study comprised 92 neonates with a median (interquartile range) LV MPI value of 0.56 (0.10) before initiation of respiratory support and 0.47 (0.04) after weaning from respiratory support with <i>P</i> < 0.001. The isovolumetric contraction time, isovolumetric relaxation time, and ejection time increased after weaning from respiratory support (all <i>P</i> < 0.0001). The severity of respiratory distress determined by invasive mode of ventilation and longer duration of respiratory support caused higher initial LV MPI before initiation of respiratory support compared with recovery and <i>P</i> < 0.001, suggesting subclinical ventricular dysfunction with respiratory distress in neonates.</p><p><strong>Conclusion: </strong>LV MPI was higher in neonates with respiratory distress and normalized after weaning from respiratory support, which indicates that neonates requiring respiratory support may have subclinical ventricular dysfunction and should be followed up carefully.</p>\",\"PeriodicalId\":8026,\"journal\":{\"name\":\"Annals of Pediatric Cardiology\",\"volume\":\"17 5\",\"pages\":\"331-338\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737619/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Pediatric Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/apc.apc_167_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Pediatric Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/apc.apc_167_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/24 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Comparing the tissue Doppler-derived left ventricular myocardial performance index before and after recovery from respiratory distress in neonates: A prospective observational study.
Background and objective: Respiratory distress is the most common cause requiring neonatal intensive care unit admission. As respiratory and cardiac functions are closely interrelated, some cardiac dysfunction is expected in respiratory distress. The myocardial performance index (MPI) is an index to assess global myocardial function, easily measurable by bedside echocardiography and reliable. Here, we conducted this study to determine the change in cardiac function in neonates with respiratory distress before initiating respiratory support and after weaning from the support.
Methodology: The study was carried out in 92 neonates with a gestational age of more than 32 weeks who required invasive or noninvasive respiratory support. The tissue Doppler left ventricular MPI (LV MPI) was calculated before the initiation of respiratory support and after weaning from respiratory support. The data were analyzed using a paired t-test and a Wilcoxon signed-rank test.
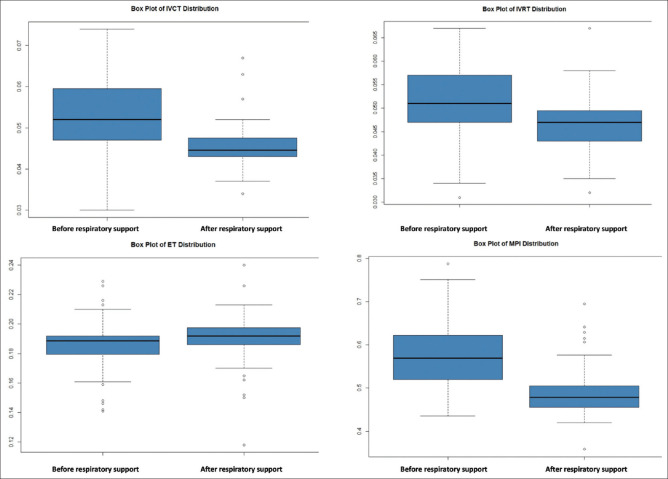
Results: This study comprised 92 neonates with a median (interquartile range) LV MPI value of 0.56 (0.10) before initiation of respiratory support and 0.47 (0.04) after weaning from respiratory support with P < 0.001. The isovolumetric contraction time, isovolumetric relaxation time, and ejection time increased after weaning from respiratory support (all P < 0.0001). The severity of respiratory distress determined by invasive mode of ventilation and longer duration of respiratory support caused higher initial LV MPI before initiation of respiratory support compared with recovery and P < 0.001, suggesting subclinical ventricular dysfunction with respiratory distress in neonates.
Conclusion: LV MPI was higher in neonates with respiratory distress and normalized after weaning from respiratory support, which indicates that neonates requiring respiratory support may have subclinical ventricular dysfunction and should be followed up carefully.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


