Luke Stanisce, Donald H Solomon, Liam O'Neill, Nadir Ahmad, Brian Swendseid, Gregory J Kubicek, Yekaterina Koshkareva
{"title":"接受多学科头颈癌治疗的服务不足患者群体的交通考虑。","authors":"Luke Stanisce, Donald H Solomon, Liam O'Neill, Nadir Ahmad, Brian Swendseid, Gregory J Kubicek, Yekaterina Koshkareva","doi":"10.3934/publichealth.2024058","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Underinsured patients with advanced head and neck cancer experience worse outcomes compared to their well-insured peers.</p><p><strong>Methods: </strong>Retrospective logistic regression analysis testing associations between demographic, geospatial, transportation, disease, and treatment factors in 50 government insured or uninsured patients receiving curative-intent, multidisciplinary cancer care.</p><p><strong>Results: </strong>Forty percent of patients missed at least one treatment or surveillance appointment within the first year. Thirty-two percent reported using public transportation; 42% relied on caregivers. Patients who used public transportation were 3.3 and 4.6 times more likely to miss treatment (p = 0.001) and surveillance (p = 0.014) visits, respectively. The median one-way travel duration for such routes was 52 minutes (range: 16-232 minutes) and included 0.7 miles of walking. Physical distance to care was not associated with transportation type, missed appointments, or disease recurrence.</p><p><strong>Conclusions: </strong>Underserved, underinsured patient populations face significant logistical challenges with transportation, which may be mitigated by alternative models of care delivery, such as multidisciplinary clinics.</p>","PeriodicalId":45684,"journal":{"name":"AIMS Public Health","volume":"11 4","pages":"1125-1136"},"PeriodicalIF":2.7000,"publicationDate":"2024-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717547/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transportation considerations in underserved patient populations receiving multidisciplinary head and neck cancer care.\",\"authors\":\"Luke Stanisce, Donald H Solomon, Liam O'Neill, Nadir Ahmad, Brian Swendseid, Gregory J Kubicek, Yekaterina Koshkareva\",\"doi\":\"10.3934/publichealth.2024058\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Underinsured patients with advanced head and neck cancer experience worse outcomes compared to their well-insured peers.</p><p><strong>Methods: </strong>Retrospective logistic regression analysis testing associations between demographic, geospatial, transportation, disease, and treatment factors in 50 government insured or uninsured patients receiving curative-intent, multidisciplinary cancer care.</p><p><strong>Results: </strong>Forty percent of patients missed at least one treatment or surveillance appointment within the first year. Thirty-two percent reported using public transportation; 42% relied on caregivers. Patients who used public transportation were 3.3 and 4.6 times more likely to miss treatment (p = 0.001) and surveillance (p = 0.014) visits, respectively. The median one-way travel duration for such routes was 52 minutes (range: 16-232 minutes) and included 0.7 miles of walking. Physical distance to care was not associated with transportation type, missed appointments, or disease recurrence.</p><p><strong>Conclusions: </strong>Underserved, underinsured patient populations face significant logistical challenges with transportation, which may be mitigated by alternative models of care delivery, such as multidisciplinary clinics.</p>\",\"PeriodicalId\":45684,\"journal\":{\"name\":\"AIMS Public Health\",\"volume\":\"11 4\",\"pages\":\"1125-1136\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-12-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717547/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AIMS Public Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3934/publichealth.2024058\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AIMS Public Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3934/publichealth.2024058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
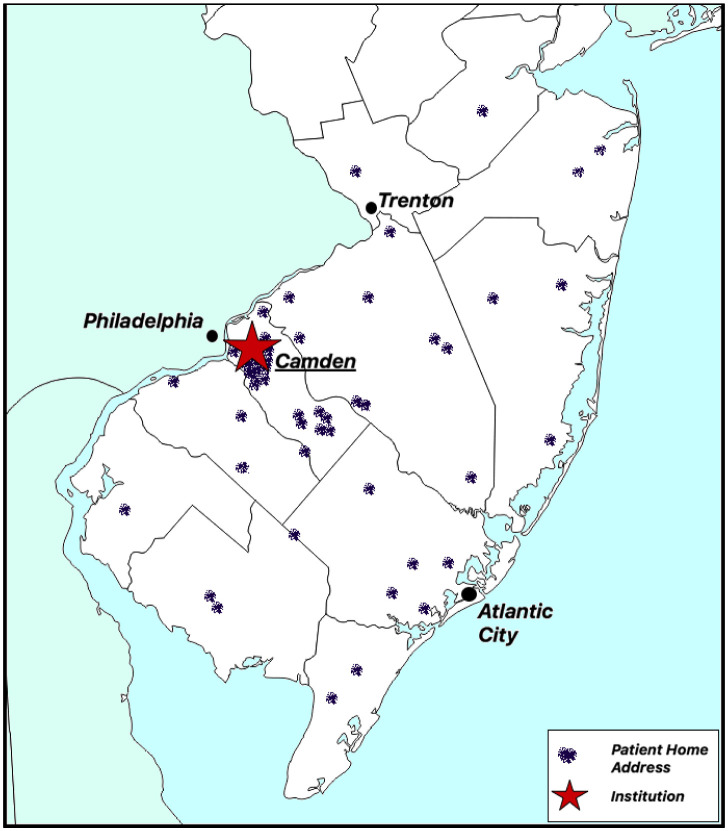
Transportation considerations in underserved patient populations receiving multidisciplinary head and neck cancer care.
Background: Underinsured patients with advanced head and neck cancer experience worse outcomes compared to their well-insured peers.
Methods: Retrospective logistic regression analysis testing associations between demographic, geospatial, transportation, disease, and treatment factors in 50 government insured or uninsured patients receiving curative-intent, multidisciplinary cancer care.
Results: Forty percent of patients missed at least one treatment or surveillance appointment within the first year. Thirty-two percent reported using public transportation; 42% relied on caregivers. Patients who used public transportation were 3.3 and 4.6 times more likely to miss treatment (p = 0.001) and surveillance (p = 0.014) visits, respectively. The median one-way travel duration for such routes was 52 minutes (range: 16-232 minutes) and included 0.7 miles of walking. Physical distance to care was not associated with transportation type, missed appointments, or disease recurrence.
Conclusions: Underserved, underinsured patient populations face significant logistical challenges with transportation, which may be mitigated by alternative models of care delivery, such as multidisciplinary clinics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


