Javier Ramos-Maqueda, Mercedes Cabrera-Ramos, Jorge Melero-Polo, Isabel Montilla-Padilla, Adrián Riaño-Ondiviela, José Ramón Ruiz-Arroyo
{"title":"左束支区起搏与右室流出道间隔起搏:中期结果和学习曲线。","authors":"Javier Ramos-Maqueda, Mercedes Cabrera-Ramos, Jorge Melero-Polo, Isabel Montilla-Padilla, Adrián Riaño-Ondiviela, José Ramón Ruiz-Arroyo","doi":"10.19102/icrm.2024.15123","DOIUrl":null,"url":null,"abstract":"<p><p>Our study evaluated the efficacy and feasibility of left bundle branch area pacing (LBBAP) compared to right ventricular outflow tract septal pacing (RVOSP). We conducted a prospective, single-center, observational study involving 200 consecutive patients who required pacemaker implantation. The patients were divided into two groups (LBBAP and RVOSP), with 100 patients in each group. We aimed to compare the safety and efficacy, as well as the procedure and fluoroscopy times, between the two groups. Additionally, we aimed to describe the learning curve for the LBBAP group. The success and acute complication rates were similar (<i>P</i> = .56 vs. <i>P</i> = .65). The procedure time was longer in the LBBAP group compared to the RVOSP group (18 [13-28] vs. 11 [7-17] min; <i>P</i> < .001), while the fluoroscopy time was shorter in the LBBAP group compared to the RVOSP group (2.8 [1.3-3.7] vs. 3.1 [2-5.9] min; <i>P</i> = .02). The paced QRS interval was narrower in the LBBAP group (123.77 ± 10.25 vs. 159.79 ± 17.0 ms; <i>P</i> = .001). There were no significant differences in pacing parameters like R-wave sensing (9.6 ± 5.2 vs. 9.1 ± 4.7 mV; <i>P</i> = .91), bipolar impedance (685.9 ± 151.8 vs. 686.5 ± 158.6 Ω; <i>P</i> = .98), or pacing threshold (0.70 ± 0.29 vs. 0.64 ± 0.26 V @ 0.4 ms; <i>P</i> = .63). In the LBBAP group, both the procedure time (12 [10.5-15] vs. 32 [28.5-38.5] min; <i>P</i> < .001) and the fluoroscopy time (2 [1-4.6] vs. 5.1 [3.4-12] min; <i>P</i> < .01) were shorter in the last quartile (Q4) compared to the first quartile (Q1). The procedure time was similar between LBBAP Q4 and RVOSP (12 [10.5-15] vs. 11 [7-17] min; <i>P</i> = .33). LBBAP is as safe as RVOSP and achieves a narrower paced QRS compared to RVOSP. After a rapid learning curve, a shorter fluoroscopy time and a similar procedure time can be achieved.</p>","PeriodicalId":36299,"journal":{"name":"Journal of Innovations in Cardiac Rhythm Management","volume":"15 12","pages":"6113-6121"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717158/pdf/","citationCount":"0","resultStr":"{\"title\":\"Left Bundle Branch Area Pacing Compared to Right Ventricular Outflow Tract Septal Pacing: Mid-term Results and Learning Curve.\",\"authors\":\"Javier Ramos-Maqueda, Mercedes Cabrera-Ramos, Jorge Melero-Polo, Isabel Montilla-Padilla, Adrián Riaño-Ondiviela, José Ramón Ruiz-Arroyo\",\"doi\":\"10.19102/icrm.2024.15123\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Our study evaluated the efficacy and feasibility of left bundle branch area pacing (LBBAP) compared to right ventricular outflow tract septal pacing (RVOSP). We conducted a prospective, single-center, observational study involving 200 consecutive patients who required pacemaker implantation. The patients were divided into two groups (LBBAP and RVOSP), with 100 patients in each group. We aimed to compare the safety and efficacy, as well as the procedure and fluoroscopy times, between the two groups. Additionally, we aimed to describe the learning curve for the LBBAP group. The success and acute complication rates were similar (<i>P</i> = .56 vs. <i>P</i> = .65). The procedure time was longer in the LBBAP group compared to the RVOSP group (18 [13-28] vs. 11 [7-17] min; <i>P</i> < .001), while the fluoroscopy time was shorter in the LBBAP group compared to the RVOSP group (2.8 [1.3-3.7] vs. 3.1 [2-5.9] min; <i>P</i> = .02). The paced QRS interval was narrower in the LBBAP group (123.77 ± 10.25 vs. 159.79 ± 17.0 ms; <i>P</i> = .001). There were no significant differences in pacing parameters like R-wave sensing (9.6 ± 5.2 vs. 9.1 ± 4.7 mV; <i>P</i> = .91), bipolar impedance (685.9 ± 151.8 vs. 686.5 ± 158.6 Ω; <i>P</i> = .98), or pacing threshold (0.70 ± 0.29 vs. 0.64 ± 0.26 V @ 0.4 ms; <i>P</i> = .63). In the LBBAP group, both the procedure time (12 [10.5-15] vs. 32 [28.5-38.5] min; <i>P</i> < .001) and the fluoroscopy time (2 [1-4.6] vs. 5.1 [3.4-12] min; <i>P</i> < .01) were shorter in the last quartile (Q4) compared to the first quartile (Q1). The procedure time was similar between LBBAP Q4 and RVOSP (12 [10.5-15] vs. 11 [7-17] min; <i>P</i> = .33). LBBAP is as safe as RVOSP and achieves a narrower paced QRS compared to RVOSP. After a rapid learning curve, a shorter fluoroscopy time and a similar procedure time can be achieved.</p>\",\"PeriodicalId\":36299,\"journal\":{\"name\":\"Journal of Innovations in Cardiac Rhythm Management\",\"volume\":\"15 12\",\"pages\":\"6113-6121\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11717158/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Innovations in Cardiac Rhythm Management\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.19102/icrm.2024.15123\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Innovations in Cardiac Rhythm Management","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.19102/icrm.2024.15123","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
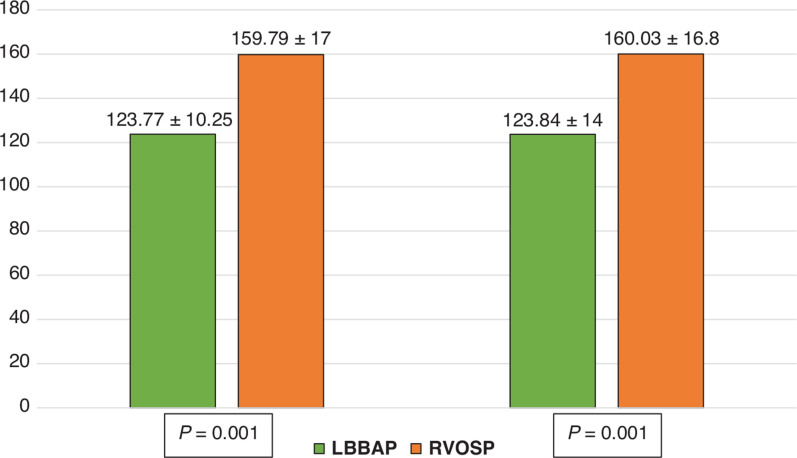
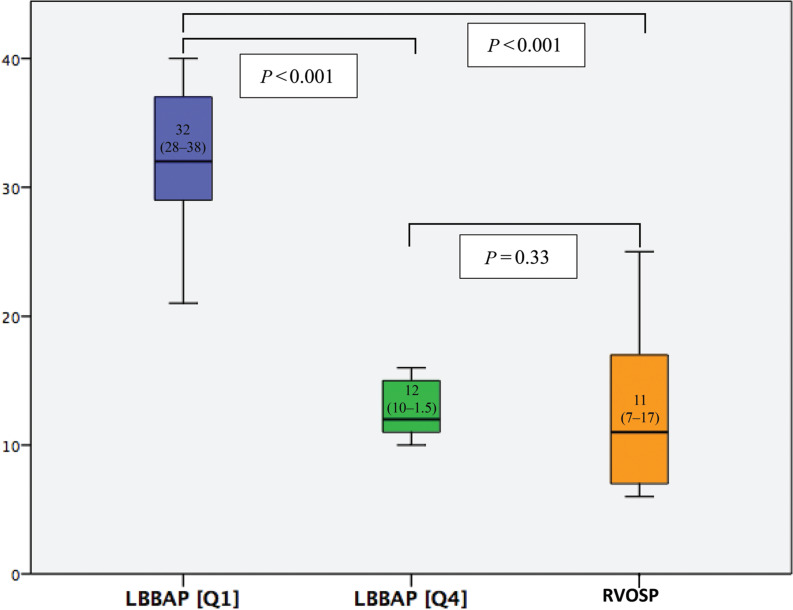
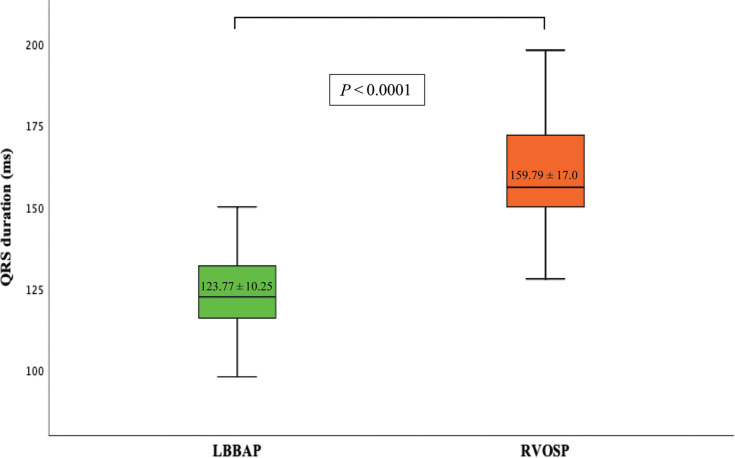
我们的研究评估了左束分支区起搏(LBBAP)与右心室流出道间隔起搏(RVOSP)的有效性和可行性。我们进行了一项前瞻性、单中心、观察性研究,涉及200名需要植入起搏器的连续患者。患者分为两组(LBBAP和RVOSP),每组100例。我们的目的是比较两组之间的安全性和有效性,以及程序和透视时间。此外,我们旨在描述LBBAP组的学习曲线。成功率和急性并发症发生率相似(P = 0.56 vs. P = 0.65)。与RVOSP组相比,LBBAP组的手术时间更长(18 [13-28]vs. 11 [7-17] min;P < 0.001),而LBBAP组透视时间较RVOSP组短(2.8 [1.3-3.7]vs. 3.1 [2-5.9] min;P = .02)。LBBAP组节律性QRS间期较短(123.77±10.25 vs 159.79±17.0 ms);P = .001)。两组的起搏参数如r波感应(9.6±5.2 vs 9.1±4.7 mV;P = 0.91),双极阻抗(685.9±151.8 vs. 686.5±158.6 Ω;P = 0.98),或起搏阈值(0.70±0.29 vs. 0.64±0.26 V @ 0.4 ms;P = .63)。在LBBAP组,手术时间分别为12 [10.5-15]vs. 32 [28.5-38.5] min;P < 0.001)和透视时间(2 [1-4.6]vs. 5.1 [3.4-12] min;P < 0.01),最后四分位数(Q4)比第一个四分位数(Q1)短。LBBAP Q4和RVOSP的手术时间相似(12 [10.5-15]vs. 11 [7-17] min;P = .33)。LBBAP与RVOSP一样安全,并且比RVOSP实现更窄的QRS。经过快速的学习曲线,可以实现更短的透视时间和类似的手术时间。
Left Bundle Branch Area Pacing Compared to Right Ventricular Outflow Tract Septal Pacing: Mid-term Results and Learning Curve.
Our study evaluated the efficacy and feasibility of left bundle branch area pacing (LBBAP) compared to right ventricular outflow tract septal pacing (RVOSP). We conducted a prospective, single-center, observational study involving 200 consecutive patients who required pacemaker implantation. The patients were divided into two groups (LBBAP and RVOSP), with 100 patients in each group. We aimed to compare the safety and efficacy, as well as the procedure and fluoroscopy times, between the two groups. Additionally, we aimed to describe the learning curve for the LBBAP group. The success and acute complication rates were similar (P = .56 vs. P = .65). The procedure time was longer in the LBBAP group compared to the RVOSP group (18 [13-28] vs. 11 [7-17] min; P < .001), while the fluoroscopy time was shorter in the LBBAP group compared to the RVOSP group (2.8 [1.3-3.7] vs. 3.1 [2-5.9] min; P = .02). The paced QRS interval was narrower in the LBBAP group (123.77 ± 10.25 vs. 159.79 ± 17.0 ms; P = .001). There were no significant differences in pacing parameters like R-wave sensing (9.6 ± 5.2 vs. 9.1 ± 4.7 mV; P = .91), bipolar impedance (685.9 ± 151.8 vs. 686.5 ± 158.6 Ω; P = .98), or pacing threshold (0.70 ± 0.29 vs. 0.64 ± 0.26 V @ 0.4 ms; P = .63). In the LBBAP group, both the procedure time (12 [10.5-15] vs. 32 [28.5-38.5] min; P < .001) and the fluoroscopy time (2 [1-4.6] vs. 5.1 [3.4-12] min; P < .01) were shorter in the last quartile (Q4) compared to the first quartile (Q1). The procedure time was similar between LBBAP Q4 and RVOSP (12 [10.5-15] vs. 11 [7-17] min; P = .33). LBBAP is as safe as RVOSP and achieves a narrower paced QRS compared to RVOSP. After a rapid learning curve, a shorter fluoroscopy time and a similar procedure time can be achieved.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


